
当科では耳、鼻、のどの基本的な病気の治療を行うとともに、神戸市民の医療の最後の砦として、多くの医療機関から患者さんのご紹介をいただき、当院でなくてはできない高度の専門的診療も行っています。また、当院では救急・救命センターが24時間、365日休まず稼働しており、急病や手術後のフォローに、万全の態勢で臨んでいます。つまり、当科は耳鼻咽喉科のあらゆる疾患に対する診療体制がいつでも準備されている、全国トップクラスの耳鼻咽喉科クリニックということができます。扁桃摘出術などの一般的な手術はもとより、慢性中耳炎・真珠腫性中耳炎や副鼻腔炎・前頭蓋底病変に対しても、学会より耳科手術指導医あるいは鼻科手術指導医の認定を受けた医師が高い技術をもって治療に当たります。特に高度難聴者に対する人工内耳手術は早くから導入しており、手術数は通算で930件を超えています。2020から2022年度の厚生労働省のNDBオープンデータを見ると、3年間で本邦で施行された人工内耳手術全3584件のうち、約5%にあたる178件、特に小児例においては全国手術件数1652件の6.3%に当たる105件の手術を当院で行っていることになります。当院の属する神戸医療圏の人口が本邦の人口の1.2%であることを考慮すると、これは良好な手術結果が患者さんとそのご家族に支持されていること、また小児難聴の治療に関しては全国から患者さんの紹介があるほど、各地域の耳鼻咽喉科医から高い評価を得ていることが要因と考えられます。2021年には総合聴覚センターも発足し、臨床・研究両面から難聴の克服を目指しています。
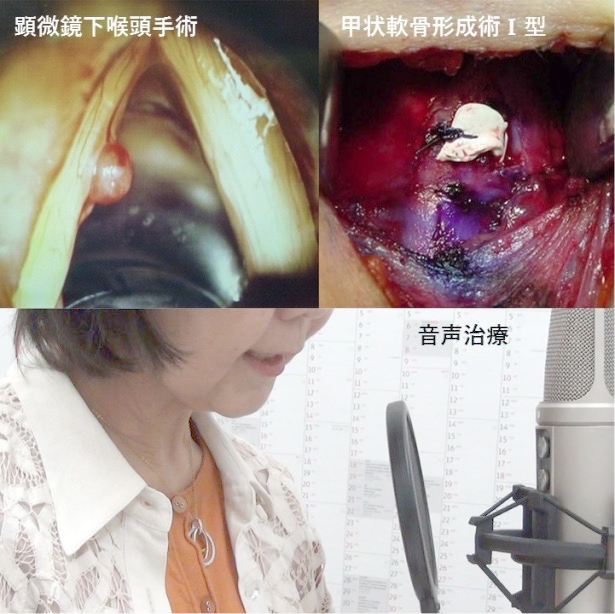
「会話」を司る音声の疾患に対しても、毎週金曜日、音声専門医と言語聴覚士がチームで治療を担当しており、ボイストレイニングを中心とした音声治療、適応があれば音声改善手術を行っており、近年ではオペラ歌手や歌劇団員など、音声を職業として使用する患者さんにも高い評価を得ています。
また、患者さんの多いめまい疾患に関しても、原因が判りにくい症例や難治症例に関しては、外部より学会認定医を招聘し、隔週月曜日に専門診療を依頼しています。
耳下腺腫瘍などの唾液腺腫瘍、舌がんなどの口腔がん、咽頭がん、喉頭がん、鼻副鼻腔がん、頭蓋底腫瘍などの耳鼻咽喉科分野の腫瘍性病変に関しては、頭頸部外科でその治療を行っております。この分野に関しては頭頸部外科のページをご参照ください。
頭頸部外科ホームページはこちら我々が安全で高い診療レベルを保てている理由は、豊富な臨床経験と多職種からなるチーム医療体制に加えて、毎週定例で行なっている診療科カンファレンスと教育的シリーズレクチャーなど、教育と研修に常に努力していることにあると思います。当科は常に、すべての手術例について事前に十分な議論を行い、それぞれの患者さんのためにベストの治療を探求しています。教育レクチャーでは当科所属の医師が、耳鼻咽喉科の中の特定の領域について調べ、カンファレンスで講義することで、診療レベルの向上を図っています。また、当科では豊富な臨床経験および臨床研究の成果を定期的に国内外の学会で発表し、その成果を記した論文は国内外の医学専門雑誌に多数掲載されています(当科および頭頸部外科の学術報告については、お知らせの欄をご参照ください)。
豊富な経験と手厚い診療体制により、患者さんのために安全で最適な治療を行うのが当科のポリシーです。


診療実績
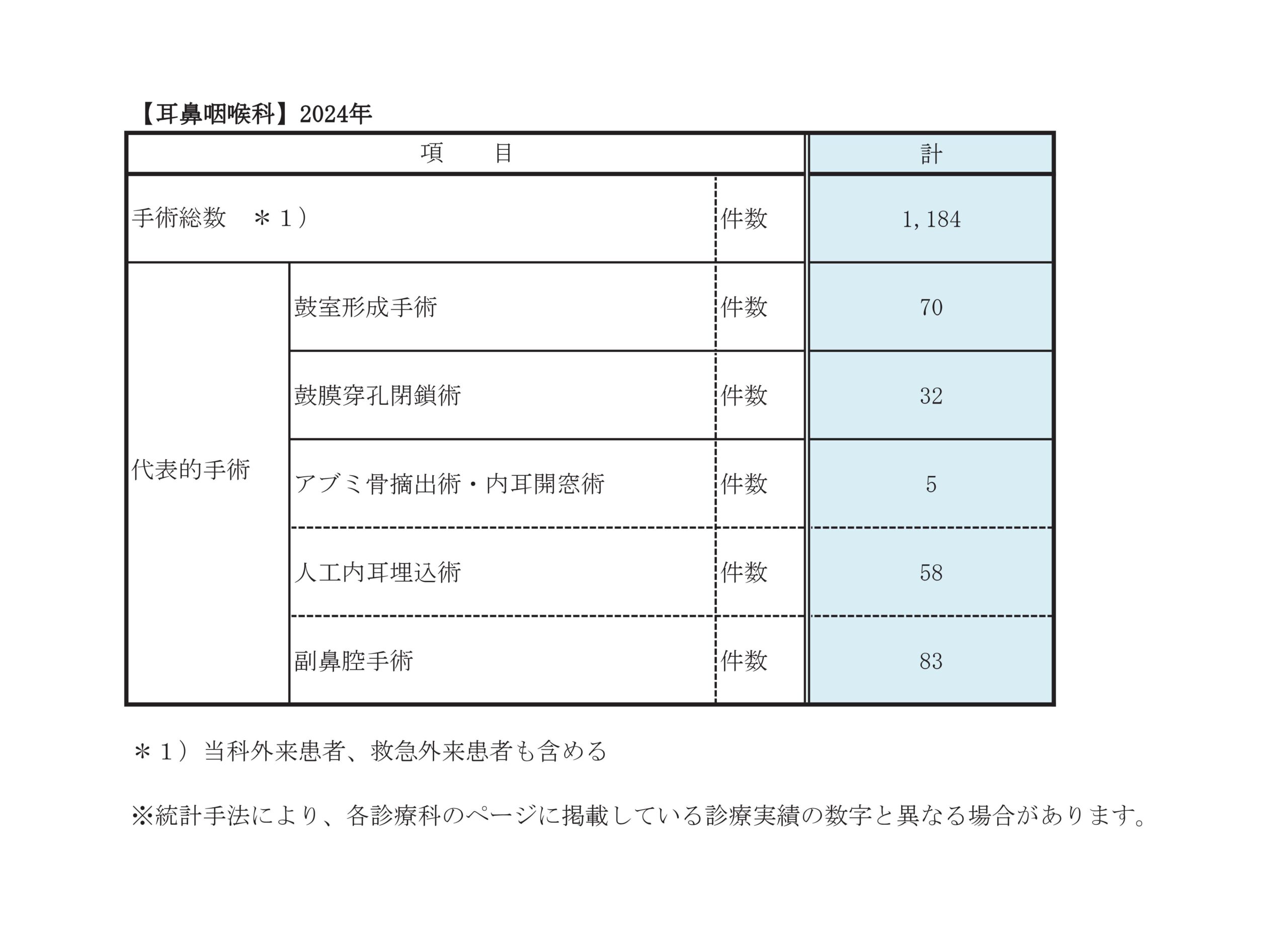
2022年~2024年 主要手術件数
| 手術名 | 2022年度 | 2023年度 | 2024年度 | |
|---|---|---|---|---|
| 耳科手術 | 308 | 300 | 284 | |
| 鼓膜形成術 | 3 | 2 | 2 | |
| 鼓膜穿孔閉鎖術 | 33 | 33 | 29 | |
| 鼓室形成術 | 71 | 66 | 65 | |
| 乳突削開術 | 24 | 21 | 29 | |
| 人工内耳手術 | 52 | 53 | 55 | |
| アブミ骨手術 | 10 | 4 | 4 | |
| 顔面神経減荷術 | 4 | 5 | 2 | |
| その他の耳科手術 | 111 | 116 | 98 | |
| 外耳道異物除去術 | 6 | 7 | 1 | |
| 鼓膜切開術 | 64 | 63 | 50 | |
| 鼓膜チューブ挿入術 | 30 | 33 | 33 | |
| 内耳窓閉鎖術 | 2 | 5 | 5 | |
| 鼻科手術総数 | 170 | 197 | 202 | |
| 内視鏡下鼻副鼻腔手術総数 | 131 | 157 | 159 | |
| 下甲介粘膜焼灼術 | 0 | 0 | 1 | |
| 内視鏡下鼻・副鼻腔手術(うち5型) | 67 | 65(3) | 61(3) | |
| 鼻副鼻腔腫瘍摘出術 | 11 | 10 | 16 | |
| 鼻副鼻腔悪性腫瘍手術 | 1 | 1 | 2 | |
| 経鼻腔的翼突管神経切除術 | 5 | 16 | 27 | |
| 内視鏡下鼻中隔手術 | 16 | 24 | 29 | |
| 内視鏡下鼻腔手術 | 27 | 35 | 21 | |
| 視神経管開放術 | 1 | 1 | 2 | |
| 内視鏡下経鼻的腫瘍摘出術 | 1 | 4 | 0 | |
| 髄液瘻閉鎖術 | 2 | 0 | 0 | |
| 涙嚢鼻腔吻合術 | 0 | 1 | 0 | |
| 鼻腔粘膜焼灼術 | 20 | 38 | 26 | |
| 鼻内異物摘出術 | 0 | 0 | 3 | |
| アデノイド切除術 | 11 | 15 | 23 | |
| 口蓋扁桃手術 | 78 | 142 | 190 | |
| 舌扁桃切除術 | 0 | 0 | 1 | |
| 喉頭微細手術 | 34 | 39 | 35 | |
| 喉頭・声帯ポリープ切除術 | 11 | 9 | 13 | |
| 喉頭腫瘍摘出術(直達鏡によるもの) | 21 | 28 | 20 | |
| 喉頭異物摘出術(直達鏡によるもの) | 0 | 1 | 2 | |
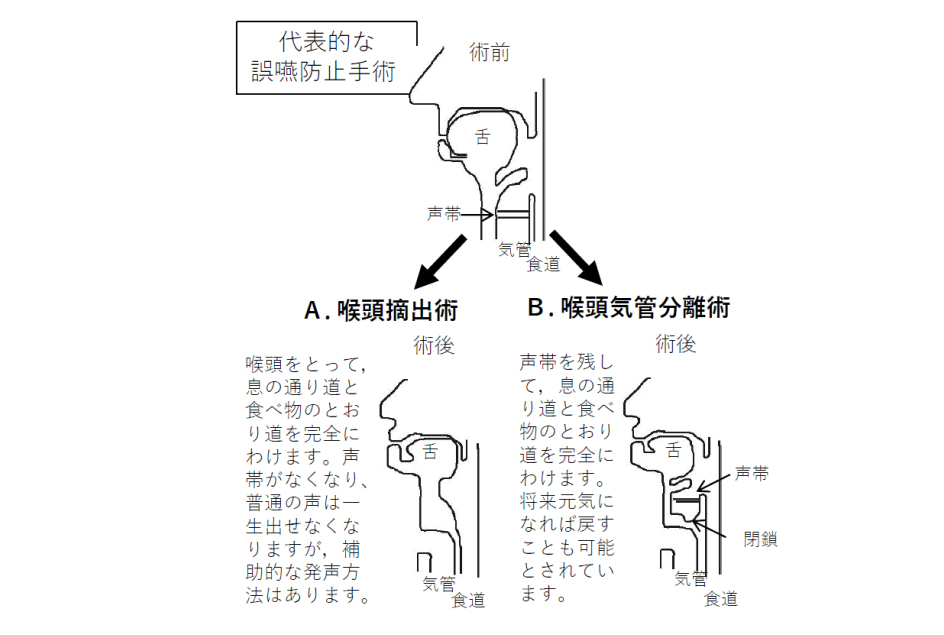
| 嚥下機能改善、誤嚥防止、音声機能改善手術 | 38 | 49 | 62 | |
| 内喉頭筋内注入術(ボツリヌス毒素) | 3 | 11 | 16 | |
| 気管切開孔閉鎖術 | 12 | 4 | 7 | |
| 喉頭形成手術 | 8 | 6 | 4 | |
| 嚥下機能手術 | 2 | 4 | 8 | |
| 軟口蓋形成手術 | 2 | 3 | 3 | |
| 気管切開術 | 76 | 72 | 54 | |
| その他の口腔咽頭手術 | 29 | 34 | 48 | |
| 咽後膿瘍切開術 | 1 | 0 | 1 | |
| 扁桃周囲膿瘍切開術 | 4 | 3 | 7 | |
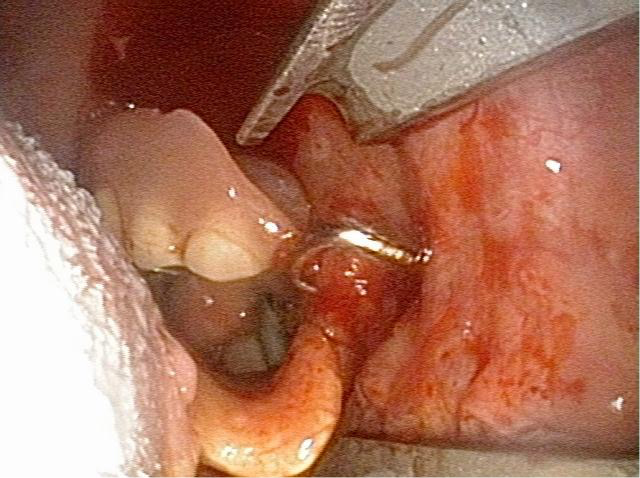
| 咽頭異物摘出術 | 18 | 10 | 21 | |
| 過長茎状突起切断術 | 1 | 0 | 3 | |
| 喉頭膿瘍切開術 | 0 | 9 | 0 | |
| 深頸部膿瘍切開術 | 4 | 0 | 15 | |
| 喉頭異物摘出術(直達鏡によらないもの) | 1 | 1 | 1 | |
| 頬・口唇・舌小帯形成手術 | 0 | 1 | 0 | |
| 手術総数(頭頸部外科を含む) | 1120 | 1310 | 1312 | |
診療科別統計
主な疾患・治療法
小児人工内耳のリハビリテーション

我々は日本耳鼻咽喉科頭頸部外科学会のガイドラインに基づき、人工内耳手術や残存聴力活用型人工内耳手術を積極的に行っています。特に、療育的観点から必要と判断される場合には同日両側耳人工内耳手術も行い好成績を得ています。
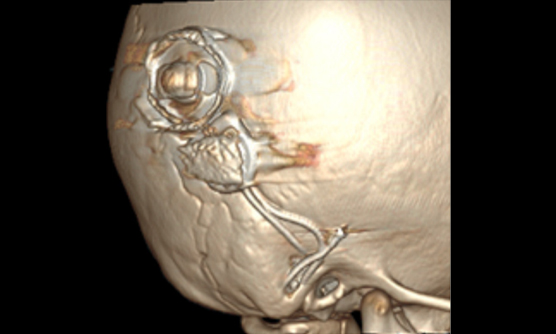
当科は経験豊富な専門医と人工内耳専任の言語聴覚士による手厚い診療体制が大きな特長で、我が国を代表する人工内耳センターの一つとなっています。
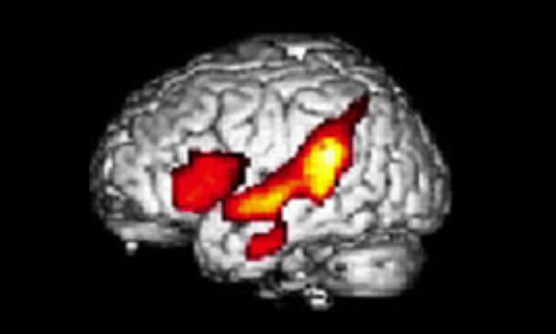
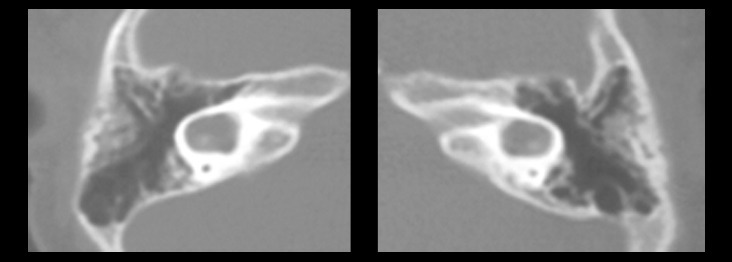
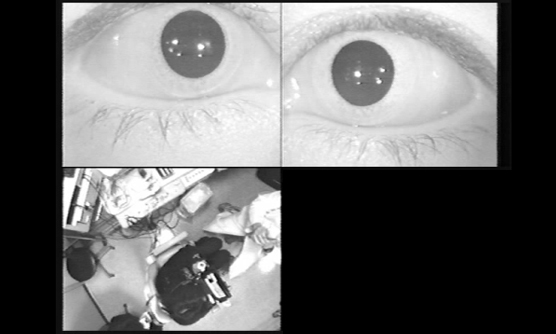
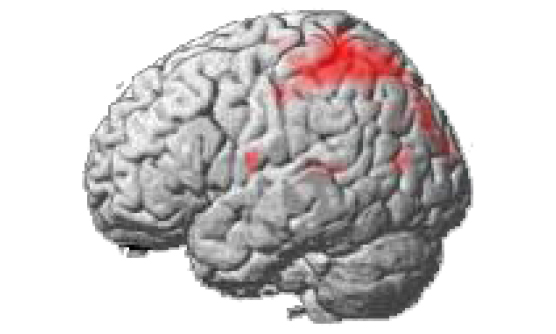
左の写真は1歳の子供さんの右人工内耳の3次元CT像(上)と、成人が右耳の人工内耳で言葉を聞いている時の脳機能画像(下:Tateya I, Naito Y, Hirano S, et al. Neuroreport, 2003より )です。
成人人工内耳のリハビリテーション
人工内耳の聴こえは、直接神経を刺激するため、本来は機械的に合成された音です。今まで記憶している音、補聴器の音とはちがう新しい聞こえになります。しかし、成人の方の場合は、脳にことばの記憶がありますので、新しい人工内耳のきこえと脳のことばの記憶を結びつけることで、だんだんと言葉が聞き取れるようになってきます。人工内耳でことばを聴くときは、意欲、注意力、推測力など多くの脳の機能で補って頭で考えて聴くようにします。集中して、推測しながらことばをたくさん聴くことで、時間の経過とともに言葉が理解できるようになってきます。
成人人工内耳術後のリハビリテーションでは、マッピングといわれる人工内耳の機器調整と聴こえの練習を行います。機器調整は言語聴覚士と一緒に、専用のパソコンで一人一人に合わせて人工内耳の聞こえを調整します。聴こえの練習は、身の回りの音を意識して聴く、ことばを聴き取り理解する、会話をする、テレビや電話も人工内耳で聞いてみるということを病院や自宅でそれぞれのペースにあわせて練習していきます。

副鼻腔真菌症に対してはハイドロデブリッダー(高圧洗浄器)を使用して効率の良い治療を行い、外傷例では、形成外科と合同で外鼻形成術や鼻中隔矯正術も行っています。より高度な技術を要する拡大副鼻腔手術(両側前頭洞単洞化手術、頭蓋底手術)も他科と連携して取り組んでいます。
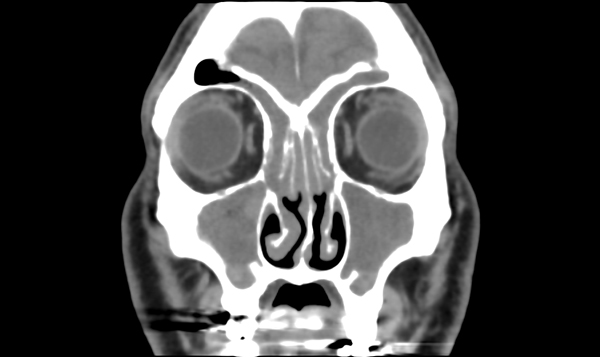
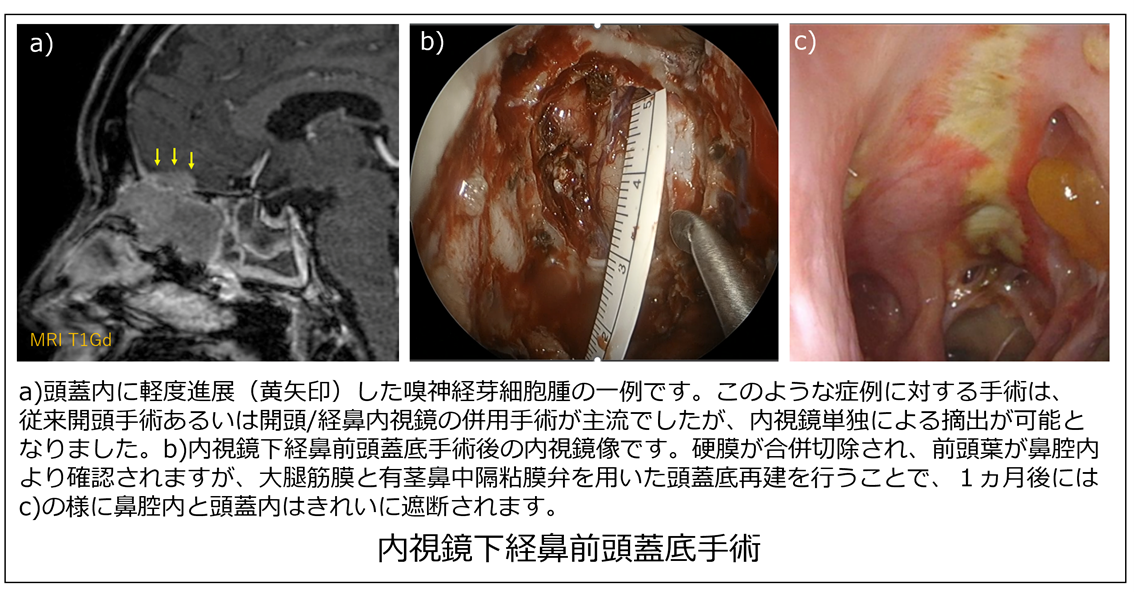
鼻副鼻腔・頭蓋底は、周囲に脳・眼窩・内頸動脈という重要な構造物が存在する解剖学的に複雑な領域ですが、同領域には良悪性含め様々な種類の腫瘍が発生します。治療の主体は手術療法ですが、悪性腫瘍及び顔面深部に発生する良性腫瘍に対する手術は、従来開頭や顔面切開による侵襲的なアプローチ法が主流でした。しかし近年では、機器や技術の発達により悪性腫瘍に対しても低侵襲な内視鏡下経鼻アプローチが試みられるようになってきています。
当院では、頭頸部外科において、早期の鼻副鼻腔がんや嗅神経芽細胞腫などの前頭蓋底悪性腫瘍に対して経鼻内視鏡下鼻副鼻腔悪性腫瘍手術・内視鏡下経鼻前頭蓋底手術(図)を行い、開頭や顔面切開を行わない低侵襲手術を行っています。また、翼口蓋窩や側頭下窩などの顔面深部に発生する腫瘍に対しては、内視鏡下経鼻手術単独あるいは小さな顔面切開との併用手術により、顔面や頭部の傷を作らないあるいは最小限の傷での手術を行っています。
頭頸部外科では、頭頸部がん指導医と鼻科手術指導医の双方の資格を有する医師が中心となり、内視鏡下経鼻アプローチで低侵襲に、かつ治療の根治性を失わない確実な切除をめざした内視鏡下経鼻手術に取り組んでいます。
一方で、進行鼻副鼻腔がんや進行頭蓋底悪性腫瘍に対しては、従来の外切開アプローチに内視鏡下経鼻手術を併用することで、切除断端が陽性となりやすい深部の切除マージンを確実につけることで手術成績の向上を図っています。脳に浸潤している場合は、脳神経外科と合同で手術を行っています。
疾患・検査・治療法の概要
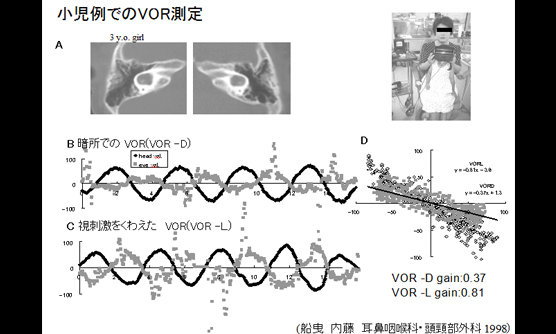
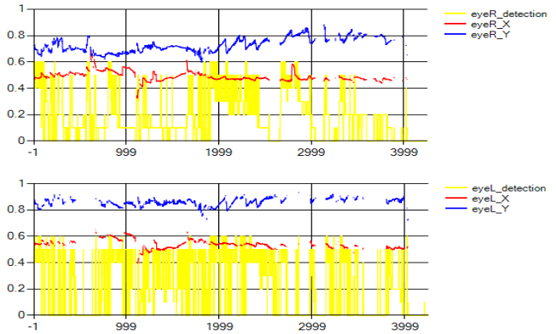
耳鼻科関連の疾患が疑われ、後に耳鼻科を受診される患者さんはそのうち約20%ほど、神経内科は14%ほどにあたり、最終的なめまいの原因として診断されるものはとしては、内耳に原因がある良性発作性頭位めまい症(BPPV)が最も多いです。当科のめまい外来では、多くの疾患に特異的所見が見られ確定診断に重要な頭位・頭位変換眼振検査での眼球運動を詳細に記録し、解析できるようになっています。また、良性発作性頭位めまい症、メニエール病と行った一般的なめまい疾患の診療に加えて、外リンパ瘻や上半規管裂隙症候群など外科的手術を要する疾患などを含めて専門的な診察・治療を要する疾患も中耳手術チームと連携を取りながら進めています。さらに、小児人工内耳症例での聴覚リハビリと並行して、体のバランス能力の発達も小児でも計測可能な手動回転対する前庭眼反射を測定するなどを通じて、きめ細かく行っています。
臨床研究
耳鼻咽喉科に受診中の患者さんへ臨床研究の実施に関するお知らせ
現在耳鼻咽喉科では、下記の臨床研究を実施しております。
この研究では、患者さんの日常診療で得られたデータ(情報)を利用させていただきます。
ご自身のデータがこの研究に利用されることについて、異議がある場合は、情報の利用や他の研究機関への提供をいつでも停止することができます。研究の計画や内容などについて詳しくお知りになりたい方、ご自身のデータがこの研究で利用されることについて異議のある方、その他ご質問がある方は、以下の「問い合わせ先」へご連絡ください。
| 研究科題名 | 当院責任者 | 説明文 |
| 難聴が疑われて精密検査機関・二次聴力検査機関を受診した0歳-6歳児についての社会的調査 | 山本典生 | |
|---|---|---|
| 人工内耳装用者の包括的な聴覚関連脳機能検査法の開発に資する研究 | 山本典生 | |
| 人工内耳装用者の音声リハビリテーションの開発に資する研究 | 山本典生 | |
| 難治性聴覚障害に関する調査研究 | 山本典生 |
お知らせ
医師、医師を目指す方向け当科のご紹介
※本コンテンツは、医師の方を対象とし、当医療機関についての理解を深めていただけるよう作成しているものであり、一般の方を対象とする宣伝・広告等を目的としたものではありません。
はじめまして、神戸市立医療センター中央市民病院 耳鼻咽喉科の内藤 泰(ないとう やすし)です。
当院では、2021年4月より全国でも初となる耳に特化した最先端医療を行う「総合聴覚センター」を新設いたしました。当センターでは高度難聴の乳幼児や高齢者の方に対して、一般的な治療法だけでなく、最新の臨床研究のご提案をしながら、患者さん1人1人に寄りそった治療を提供しています。
今回は、小児難聴に関する現状を踏まえた、当センターでの取組について、ご紹介いたします。
内藤 泰
総合聴覚センター 顧問
小児難聴の現状
小児の難聴は、耳の治療だけでなく、脳と言葉の発達、教育、福祉、就労支援など、様々な方向から複合的に取り組む必要があります。例えば、先天性重度難聴では人工内耳が標準的な医療として定着し、機器の進歩も続いていますが、就学前小児の療育、その後の学校教育や在学中の支援は旧来の枠組みのままであり、従来よりはるかに高度の聴覚が獲得できるようになった近年の難聴医療の進歩に追いついていません。

乳幼児期は難聴幼児通園施設あるいは普通幼稚園、小学校は普通学校、「きこえと言葉の教室」や難聴学級がある小学校あるいは聴覚特別支援学校、その後の中学校、高等学校への進学など、難聴小児には各段階で多様な選択肢があり、担当する教員や言語聴覚士などの専門職も次々に変わるので、その都度、家族は施設の選択や進学時の説明などに多大な労力を費やします。
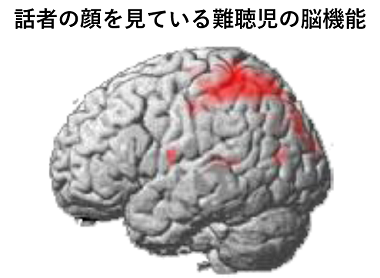
また、難聴児のコミュニケーションを音声言語だけにするのか、手話などの視覚的方法を併用するかの選択についても、判断の指標となる科学的根拠が乏しく、難聴児とその家族が途方に暮れる例が頻繁に見られます。
さらに年長になると難聴小児相互のつながりの場がなく、難聴児が孤立する例も少なくありません。
そのため、小児難聴の治療においては、単に治療を行うだけではなく、患者や患者家族が安心して治療に臨める環境を提供することが大切であると考えています。
総合聴覚センター開設の目的
このような小児難聴の現状を踏まえて、当院では、耳鼻咽喉科に新しく「総合聴覚センター」を開設しました。

このセンターでは個々の小児が最適のコミュニケーションモードを選択できるように言語発達の基盤となる脳機能の研究とリハビリテーションプログラム開発を行うとともに、難聴児やその家族がつながり、互いに支え合う場も提供したいと考えています。
また一方で、本邦は超高齢化社会となり、ほぼすべての人にとって加齢性難聴は避けて通れない問題になっています。
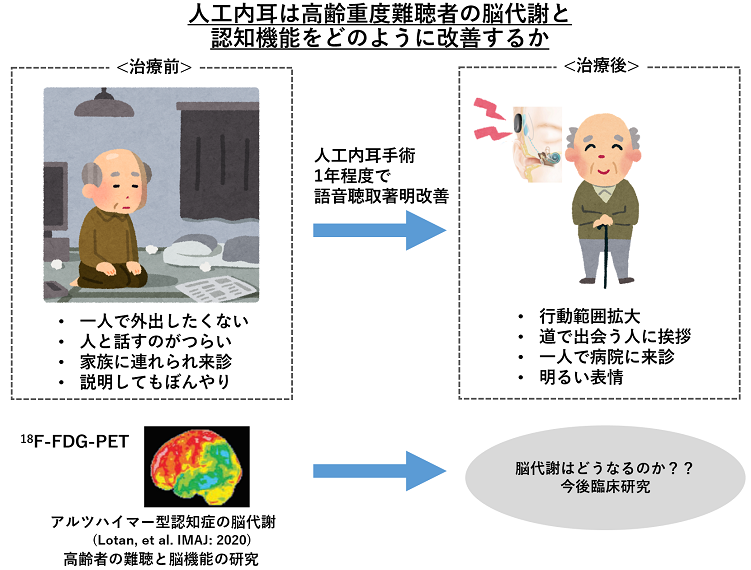
高齢者の難聴は予防可能な認知症リスクの中で最大のものとされており、日常的なコミュニケーションの障害や難聴に起因する認知機能の低下などについて、その危険性が指摘されているものの、科学的根拠は未だ示されていません。
総合聴覚センターでは、高齢者の難聴において、補聴やカウンセリング、人工内耳手術など、積極的な介入を行うとともに、その介入が脳機能のどのような改善をもたらすのかについても臨床研究を開始し、科学的根拠を提供することを目指します。
1人1人の患者さんに向き合った治療選択
当センターの取り組みは保険診療の枠組みを超えた部分があります。
当センターに患者さんをご紹介いただくと、まず一般的な保険診療の範囲で聴覚や言語発達、認知機能の検査、詳細な画像診断などを行い、その結果をご説明します。そのうえで、当科で実施している難聴に関するいくつかの臨床研究の対象となるか、そのような研究にご同意いただけるかを確かめ、条件が整った場合に臨床研究にご協力、ご参加いただくことになります。
臨床研究の対象とはならず、通常の保険診療で詳しく拝見していく患者さんも多いのであらかじめご了承をお願いします。また、臨床研究で得られる知見は、未だ大規模な臨床試験や多数の施設の追試などで確認されていない事項が含まれますので、あくまで現時点での参考所見としてご説明します。
先生方へのメッセージ
当センターでは、このような研究を通じて将来の新しい検査や治療法を創出し、医学の進歩に貢献することを目指しています。
現在、当センターが主に対象としている患者さんは高度難聴の乳幼児と高齢者(音が聞こえない、あるいは音は聞こえるが内容が分からない方)の方々です。実際には当科に受診していただいて精査しないと当センターで継続して拝見することになるかわからないことも多いので、先生方の感覚で高度の難聴が疑われる患者さんを、まず当院の地域医療連携センターを通じて耳鼻咽喉科「院外初診外来(木曜日):山本典生」宛に広くご紹介いただければ幸いです。
「神戸市は子供から高齢者まで、難聴があっても安心して活力を持って生活できる街だ」と言ってもらえるように様々な取り組みを始めますので、「総合聴覚センター」のご支援、難聴患者さんのご紹介をよろしくお願い申し上げます。
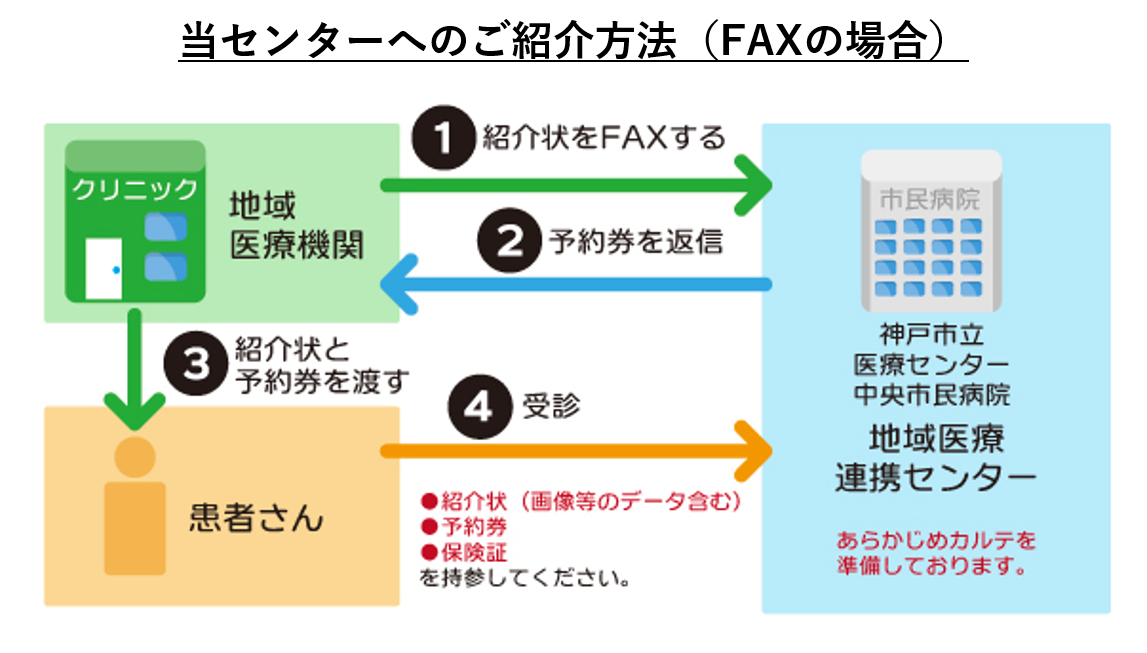
当院へのご紹介方法について
当院では、地域の医療機関の先生からご紹介いただく患者さんの待ち時間を短縮するため、診察・検査のFAX予約をお願いしております。ご紹介時には、下図のフローの通り、紹介予約をいただけますようお願いいたします。
また、連携登録医施設からのご紹介の場合は、インターネット紹介予約システムのご利用も可能です。
その他のお知らせ
新生児の聴覚検査助成について
新生児の難聴は、家庭で気付くことが難しく、そのままにしておくと言語の発達が遅れる場合があります。
神戸市では、新生児の聴覚検査の費用を助成する取り組みを2019年10月1日より開始しています。
難聴は早期に発見し、適切な療育を受けることが大切です。
概要
| 対象 | 親が市内在住で、令和元年10月1日以降に生まれた子 |
|---|---|
| 助成券の受け取り方法 | 9月以降に妊娠届を出した人は、母子健康手帳と一緒に交付。すでに母子健康手帳を持っている人は、出産予定の市内医療機関で受け取ることができます。市外で出産予定の人は、ホームページで確認を。 |
みなさまへメッセージ
新生児から乳幼児期は、言葉を覚えていく大切な時期。いろいろな言葉を聞くことは言語だけでなくコミュニケーション能力の発達にも重要です。生まれてくる全ての赤ちゃんに、公平にこの制度の恩恵を受けてほしいです。
総合聴覚センター 顧問
内藤 泰
新生児聴覚検査助成事業に関する詳細情報
神戸市HP「新生児聴覚検査費用助成事業」お問い合わせ先
神戸市総合コールセンター
TEL:078-333-3330
総合聴覚センター
総合聴覚センターホームページはこちら皆様へ
小児の難聴・聴覚障害は、早期に発見し、適切な支援を行うことが重要です。
総合聴覚センターでは神戸市からの委託を受け、医療・保健・福祉・教育の連携を強化し、聴覚障害児とその家族に対して適切な情報と切れ目のない支援を提供することを目的として、国の補助事業を活用した「聴覚障害児支援中核機能強化事業」を令和4年1月より開始しています。
以下の業務を「総合聴覚センター」で行っています。
1.事業の概要
- 聴覚障害児支援の中核機能を神戸市立医療センター中央市民病院「総合聴覚センター」に整備し、専門のコーディネーターを配置しています。
- 「総合聴覚センター」が中核となって、医療・保健・福祉・教育の関係機関が連携して、以下の事業を行います。
2.事業の内容
- 聴覚障害児支援に対する協議会を設置します。
- 聴覚障害児支援の関係機関の連携を強化。
- 聴覚障害に関する家族からの相談に応じ、検査・補聴器・人工内耳・手話等を含む適切な情報提供。
- 聴覚障害児が通う保育所・幼稚園等への巡回支援。
- 聴覚障害児の支援者を対象に、支援に関する研修等の実施。
3.問い合わせ先
神戸市立医療センター中央市民病院 耳鼻咽喉科 総合聴覚センター
078-302-4516(直通)
耳鼻咽喉科 総合聴覚センター 顧問 内藤 泰
小児の難聴は、耳の治療だけでなく、脳と言葉の発達、教育、福祉、就労支援など、様々な方向から複合的に取り組む必要があります。例えば、先天性重度難聴では人工内耳が標準的な医療として定着し、機器の進歩も続いていますが(図2)、就学前小児の療育、その後の学校教育や在学中の支援は旧来の枠組みのままであり、従来よりよりはるかに高度の聴覚が獲得できるようになった近年の難聴医療の進歩に追いついていません。乳幼児期は難聴幼児通園施設あるいは普通幼稚園、小学校は普通学校、難聴学級がある小学校あるいは聴覚特別支援学校、その後の中学校、高等学校への進学など、難聴小児には各段階で複数の選択肢があり、担当する言語聴覚士や教員などの専門職も次々に変わるので、その都度、家族は施設の選択や進学時の説明などに多大な労力を費やします。また、難聴児のコミュニケーションを音声言語だけにするのか、手話などの視覚的方法を併用するかの選択についても、判断の指標となる科学的根拠(図3)が乏しく、難聴児とその家族が途方に暮れる例が頻繁に見られます。さらに年長になると難聴小児相互のつながりの場がなく、難聴児が孤立する例も少なくありません。
今回、南館1階で新しく始める「総合聴覚センター」(図4、図5)では、個々の小児が最適のコミュニケーションモードを選択できるように言語発達の基盤となる脳機能の研究とリハビリテーションプログラム開発を行うとともに、難聴児やその家族がつながり、互いに支え合う場も提供したいと考えています。


一方、本邦は超高齢化社会となり、ほぼすべての人にとって加齢性難聴は避けて通れない問題になっています。高齢者の難聴は予防可能な認知症リスクの中で最大のものとされており、日常的なコミュニケーションの障害や難聴に起因する認知機能の低下などについて、その危険性が指摘されているものの、科学的根拠は未だ示されていません。総合聴覚センターでは、高齢者の難聴において、適切な補聴やカウンセリング、あるいは人工内耳手術など、積極的な介入を行うとともに、その介入が脳機能のどのような改善をもたらすのかについても研究し、科学的根拠を提供することを目指します。
以上、「神戸市は子供から高齢者まで、難聴があっても安心して活力を持って生活できる街だ」と言ってもらえるように頑張りますので、「総合聴覚センター」のご支援をよろしくお願いします。

