呼吸器外科は心臓・大血管・食道以外の胸部臓器を扱う外科です。主に肺がん・気胸・膿胸などの肺疾患や縦隔・胸壁腫瘍の手術のほか、胸部外傷の診療に携わります。
・真の低侵襲呼吸器外科手術
この二十年で胸腔鏡手術が呼吸器外科領域の標準術式となりました。当科ではロボット支援胸腔鏡手術や単孔式胸腔鏡手術を積極的に取り入れてゆくと同時に、手術を受けられる患者さんの体への負担、侵襲が少ない本当の意味での低侵襲胸腔鏡手術を追求してゆきます。
・断らない呼吸器外科
病院内の連携により他病院では手術を断られるような進行肺癌症例の拡大手術や救急症例の緊急手術にも積極的に取り組み、病院の総合力を患者さんに還元することを目指します。
・持続可能な呼吸器外科
病院内、科内での連携を重視し、多様性を受け入れ、若手医師、看護師、コメディカルも働きやすい持続可能な呼吸器外科を目指します。
他科・他職種と共に、綿密な治療計画と円滑な周術期管理を
呼吸器内科・外科、腫瘍内科、放射線治療科、先端医療センターとの合同カンファランスを開催し、治療方針についての検討を行っています。

術前術後の呼吸リハビリテーションを行い、術後の順調な回復のサポートを行っています。

診療実績
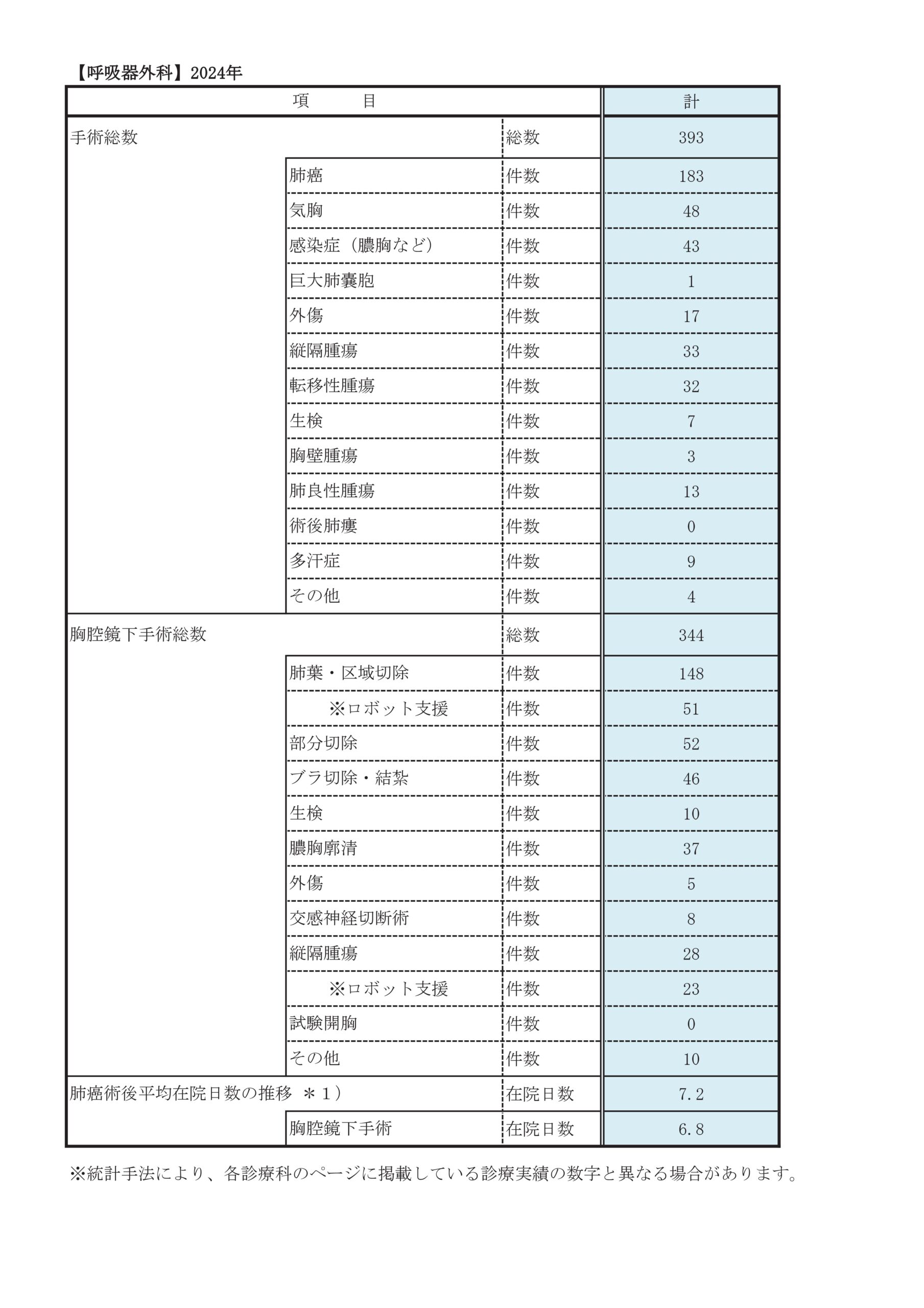
2024年手術総数:393件
| 主な疾患 | 件数 |
| 肺がん | 183例 |
|---|---|
| 気胸 | 48例 |
| 縦隔腫瘍 | 33例 |
| 感染症(膿胸など) | 43例 |
| 転移性肺腫瘍 | 32例 |
| 手掌多汗症 | 9例 |
| 外傷 | 17例 |
| 生検 | 7例 |
| 胸腔鏡手術 | 344例 |
|---|---|
| 胸腔鏡下肺葉/区域切除 | 148例 |
| 主な術式 | 件数 |
2011年以降の手術数の経年推移
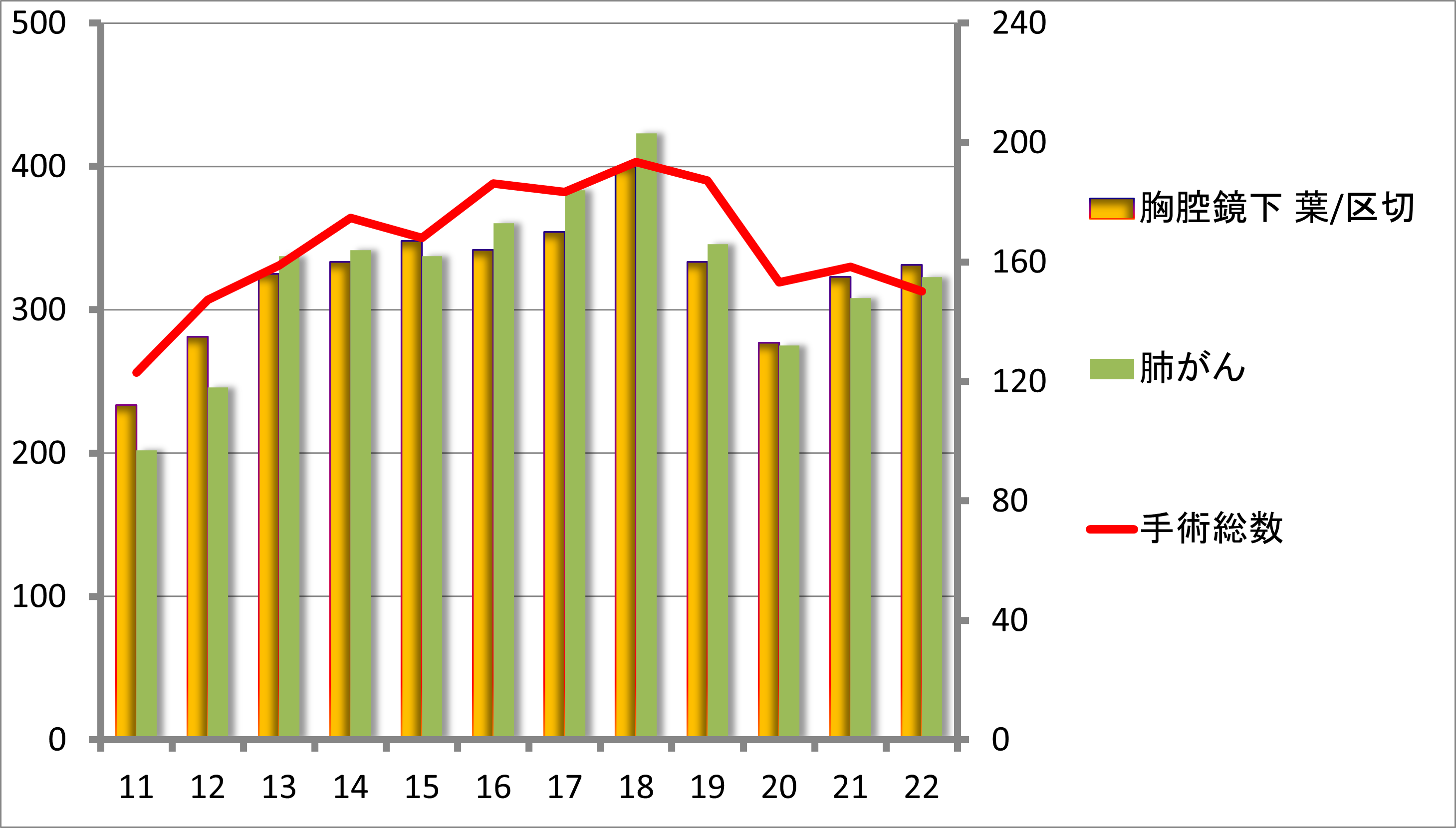
2011年以降の手術数の経年推移
肺がん治療成績
2012〜2022年の肺がん治療成績(5年生存率)
| 臨床病期別 | ⅠA期 | 86.0%(995例) | ⅠB期 | 84.8%(271例) |
|---|---|---|---|---|
| ⅡA期 | 78.8%(49例) | ⅡB期 | 61.1%(172例) | |
| ⅢA期 | 72.3%(142例) | ⅢB期 | 67.2%(37例) |
| 病理病期別 | ⅠA期 | 88.6%(942例) | ⅠB期 | 77.8%(239例) |
|---|---|---|---|---|
| ⅡA期 | 76.8%(68例) | ⅡB期 | 71.4%(191例) | |
| ⅢA期 | 65.2%(156例) | ⅢB期 | 53.5%(26例) |
診療科別統計
主な疾患・治療法
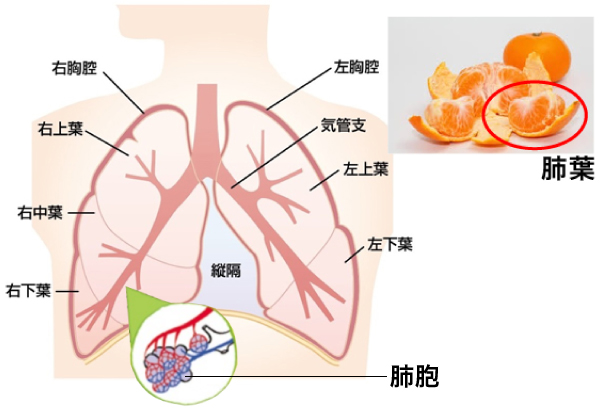
肺の構造と肺がん
肺は肋骨と横隔膜に囲まれた箱(胸腔)の中にあり、右は3つの部屋、左は2つの部屋に分かれています。その部屋は肺葉と呼ばれ、図にある蜜柑のようなイメージとなります。呼吸は空気が気管や気管支と呼ばれる通り道を移動し、末端にある肺胞と呼ばれる小さな袋構造で酸素の取り込みと二酸化炭素の排出を行うことによって行われます。肺がんはその気管支からから肺胞に至るまでのどこかで細胞ががん化したものです。肺がんの手術は、がんのある肺葉(部屋)ごと切除する肺葉切除が基本術式で、これは開胸手術、胸腔鏡下手術、ロボット支援下手術においても同じです。進行例では、2葉切除や肺全摘を要することもあり、がんの浸潤した周囲臓器(胸壁、横隔膜、上大静脈、心嚢、左房等)の合併切除も行います。一方、肺機能温存を重視した縮小手術(楔状切除・区域切除)も行っております。
肺がんに対する胸腔鏡手術
当科では肺がんに対する根治性と手術の安全性を最重視し、胸腔鏡手術を積極的に行っています。
従来の胸腔鏡手術に加えて単孔式胸腔鏡手術やロボット支援胸腔鏡手術も取り入れて、
病気の状況や根治性を考えたうえで適切な手術方法を患者さんとも相談しつつ決定しております。

肺がん診療における当科のオーダーメイド医療
当科では個々の患者さんにあった治療を検討し提案しております。具体的には肺機能温存を重視した縮小手術や、相談の上で手術を希望されない場合には放射線定位照射を行い再発(再燃)時に手術を行うことも提案しています。
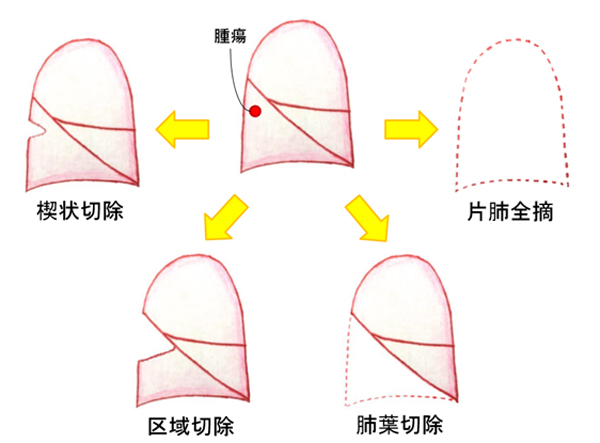
肺がんの手術には切除範囲の小さい順から下記のように4種類に分けられます。(下図「がんに対する術式」)
- 肺を部分的に切除する楔状切除(部分切除)
- 片側の肺全体を切除する一側肺全摘
- 肺葉を切除する肺葉切除
- 肺区域を切除する区域切除
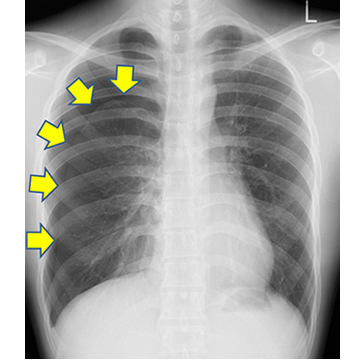
気胸、肺嚢胞とは
まれに緊張性気胸という空気漏れがどんどんひどくなり、肺や心臓を圧迫してしまう恐ろしい状態になることもあるため、胸の痛みや息苦しさを感じた際は早めに医療機関を受診することをおすすめします。
検査
多くはレントゲンで診断可能ですが、CTを撮影することでより詳細に原因検索をすることができます。また、CTで原因となるブラが見つからなくても、試験胸腔鏡といって全身麻酔下で実際に胸の中をカメラで覗くことで、他の検査ではわからないような小さなブラが見つかることもあります。

治療
保存的加療(手術を行わない治療)と手術療法があります。軽度の気胸の場合は経過観察することもありますが、中等度以上の気胸であれば管を胸に挿入し、漏れた空気を吸い出します。これだけでも治ることもありますが、再発しやすいという問題点があります。保存的加療のみであれば30-50%が再発すると言われており、手術を行うことで3-7%にまで低下します。当院では胸腔鏡下に手術を行っており、小さな創で手術を行う事ができ、術後の回復も非常に良好です。
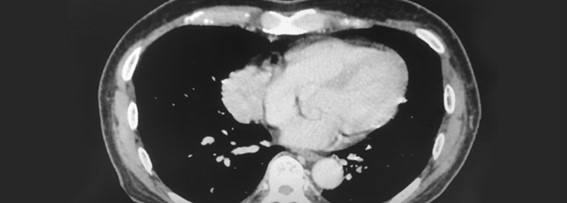
巨大肺嚢胞
胸腔内に巨大な肺嚢胞ができる病気です。正常な肺組織が圧迫され、呼吸機能が低下してしまいます。手術を行い、巨大肺嚢胞を切除することで、圧迫されていた肺が拡張し、呼吸機能の改善が期待できます。こちらも胸腔鏡下手術が可能です。
縦隔腫瘍
胸郭内において胸膜によって左右の肺に隔てられた空間を縦隔といい、縦隔内に生じる腫瘍のことです。良性の場合もあれば悪性の場合もあります(胸腺腫、胸腺癌、神経原性腫瘍、胚細胞腫瘍、悪性リンパ腫など)。検診などで偶発的に発見されることが多く、無症状の場合が多いです。
胸腺腫は最も多い縦隔腫瘍で、縦隔内にある胸腺という臓器から発生する腫瘍です。悪性度は低いのですが、放置すれば多臓器への浸潤・転移を来しますので、一般的には切除をお勧めします。
重症筋無力症
自己免疫性疾患の一つで、自己抗体である抗アセチルコリン受容体抗体が骨格筋の神経筋接合部に接合し、筋力低下などを来す疾患です。症状としては、筋力低下や易疲労性(特に夕方になると悪化)、眼瞼下垂、複視(物が二重に見える)を来します。胸腺及び周囲の脂肪組織が自己抗体の産生に関係していると考えられており、それらを一括切除します。
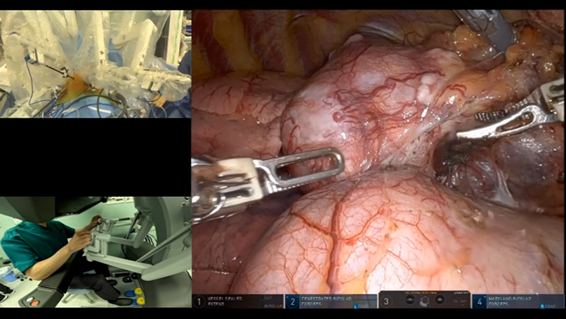
従来、縦隔腫瘍・重症筋無力症の手術は、胸骨正中切開(胸骨を縦に切開する方法、心臓手術に用いられる)で行っていましたが、当科ではロボット支援胸腔鏡手術を取り入れて胸腔鏡を用いた手術を積極的に行っています。
手術の方法には胸骨正中切開と胸腔鏡下腫瘍摘出術があります。当科では可能であれば傷が小さく済む胸腔鏡を用いてこれらの疾患の治療に当たりますが、腫瘍の状況や根治性を考えたうえで適切な治療法を患者さんと相談しつつ決定しております。

手掌多汗症の症状とその代表的な治療について
当科を訪れる手掌多汗症の方々は手汗による悩みを日々抱えておられます。大切な書類がしわになる、握手ができないなど、悩みはさまざまかつ大変な不便を感じられています。
治療には制汗剤(塩化アルミニウムなど)の外用、心理療法(カウンセリング、自律神経訓練法など)、ペインクリニック(交感神経節ブロックなど)、内服加療(漢方薬、プロ・バンサイン®:自律神経節遮断作用のある薬剤など)の他、根本治療としての手術(交感神経節切断術)があります。
当科での手掌多汗症の治療について
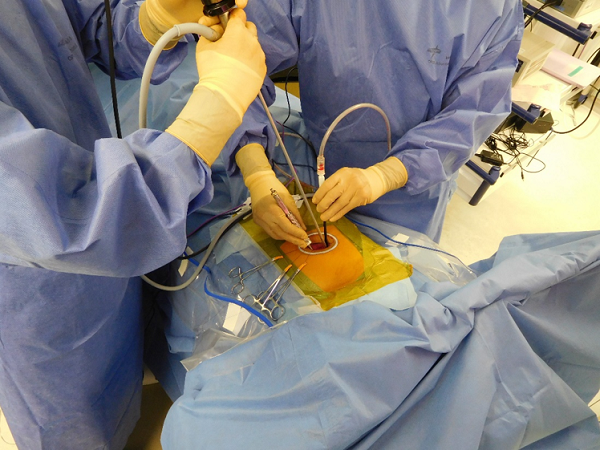
当科では根本治療を望まれる方や重症の方に対して、胸腔鏡を用いた胸腔鏡下両側交感神経節切断術を施行しています。手術は基本的には入院当日に行い、順調であれば翌日にも退院可能となります。
脇の下に5mmの皮膚切開を2か所置き、そこからカメラなどの器具を入れて目的の交感神経を見つけ、超音波凝固切開装置により切断します。
当施設ではピンポイントで神経の切断を行い、術中に効果判定を行っております。このような工夫によって確実に原因となっている交感神経のみを切断でき、必要以上に神経を切断しないことから治療効果を最大限に高め、合併症も最小限にとどめています。
手術に伴う代表的な合併症
手術を受けられる予定の方には、種々の合併症のリスクを織り込み済みであっても、現在の症状や将来のため、手掌多汗症を改善させたいかどうかを十分に考えて頂いております。
代償性発汗
手術を受けられた方には程度の差はありますがほぼ生じます。手掌から汗がでなくなる代わりに背中、腹部、下肢の発汗が増強します。一部の方では日常生活に差しさわりが生じる程度まで代償性発汗が生じる方もいます。
ホルネル症候群
神経走行が生まれつき一般的でない場合にごく稀に軽度のものが起こる可能性があります。症状としては顔面の発汗低下や瞳孔不同などですが、ほとんどが一時的であり改善します。
心臓への影響
交感神経を切断するため心拍数が約10%程度減少しますが、日常生活に支障を来す程度には至りません。
※通常の呼吸器外科の手術に比し、危険な手技はないため安全性が非常に高いです。

当科で治療を行う代表的な胸部外傷について
肋骨あるいは胸骨骨折
肋骨あるいは胸骨骨折は基本的には保存的加療のみでよいことが多い傷病です。しかし、骨折箇所が多数に及んだ場合に加え、骨折により肺、横隔膜、心臓、胸腺、肝臓、脾臓などの臓器が損傷を受けた場合や、その恐れがある場合に手術加療が必要となります。
骨折の程度によっては呼吸不全に陥ることがあり、集中治療室での管理が必要となることもあります。
また、骨折は疼痛を伴う疾病であることから、痰を喀出することが困難となり、肺炎や無気肺(肺に空気が入らない状態)といった呼吸器合併症を伴うことがあります。必要に応じて点滴、内服薬あるいは硬膜外麻酔といった様々な鎮痛を行います。
肺挫傷
胸部外傷に伴って肺胞や毛細血管の一部が断裂することによって生じます。広範囲かつ重篤な場合には呼吸不全に陥ることがあります。肺内への出血が重篤になった場合には手術加療を行うことがあります。
外傷による血胸あるいは気胸
肺や横隔膜などの胸腔内臓器が何らかの損傷を受けた場合、胸腔内には血液が貯留し、これを血胸と呼びます。また、肺外に空気が漏れることを、気胸と呼びます。これらの出血や空気により肺が圧迫されることで正常な呼吸が妨げられるため、呼吸不全に陥ることがあります。
多くは胸腔ドレーンと呼ばれるチューブによって排液あるいは排気をさせることで軽快が得られることが多いですが、その根本原因として肋骨骨折や肺損傷がある際には手術加療が必要となります。
胸部外傷に対する当科の手術の特徴
当科では積極的に胸腔鏡を用いた手術加療を行っています。状況に応じて開胸操作(従来の皮膚切開が大きい手術)を行うこともありますが、より低侵襲な手術を行うことによって、手術を受けた方がより早期に社会復帰できるよう努力しています。多くの方は手術翌日から食事摂取をとることが可能となるほか、外傷の程度によっては歩行の訓練を理学療法士の方とともに行っていただきます。
術後は点滴や酸素マスク、胸腔ドレーンなど治療に必要な管が多数ついていますが、必要がなくなれば順次抜去し、検査結果等と併せ、退院あるいはリハビリ目的の転院を目指します。
また、当科では臨床研究として、「高エネルギー胸部外傷患者における呼吸器系メカニクスに関する前向き研究」を行っており、対象となりうる患者さんにお声を掛けさせて頂き、説明の上で研究登録へのご協力をお願いしております。
主な検査内容
肺生検
間質性肺炎などの診断のため肺のごく一部を取ってきます。胸腔鏡下に行います。
縦隔鏡検査
縦隔リンパ節を採取して、がんやリンパ腫、結核・サルコイドーシスなどの診断をします。
胸膜生検
一般に肋膜と呼ばれる組織を胸腔鏡で生検します。
臨床研究
呼吸器外科の入院・外来患者さんを対象とした研究について
当科では対象となる患者さんへ文書及び口頭で説明を行い、その同意を頂いた上で検査結果や治療内容、術後の合併症など様々な臨床データの解析、研究を行っています。そしてこれらのデータは医学の発展に関して有用である場合は学会発表や医学雑誌へ投稿することを検討しています。これにより医療従事者の間で治療が奏功したデータなどを共有することが出来、より多くの患者さんに治療及び検査の恩恵を受けて頂くことが可能となると考えています。
これらの患者さんの個人情報並び臨床データは厳重に管理され、学術目的で使用する際には患者さんの氏名・住所など個人が特定できる情報は含まれません。
このような臨床研究に対して追加の説明を希望される場合、また個人の臨床データのデータベースへの収集及び臨床研究への活用を拒否される場合には担当医師まで何時でも遠慮なくお申し出ください。また、これらの同意に関して発表あるいは投稿前であればいつでも撤回が可能であり、撤回をすることによる患者さんへの不利益は一切生じません。
詳細に関しましてはこちら(当院の臨床研究推進センター )をご覧ください。現在以下の臨床研究を行っております。
| 研究課題名 | 当院責任者 | 承認日 | 説明文 (PDF) |
| 病理病期IA2-IIA期EGFR遺伝子変異陽性非小細胞肺癌における術後補助療法の実態を調査する多施設共同前向き観察研究 | 山田徹 |
2024年9月17日 |
|
|---|---|---|---|
| EGFR遺伝子変異陽性非小細胞肺癌完全切除例の前向き観察研究 | 山田徹 |
2025年2月4日 |
|
| 当院における間質性肺炎合併肺癌の治療成績 | 栢分秀直 | 2024年1月17日 | |
| 手掌多汗症手術におけるリアルタイム体温モニターの有用性 | 鉄本啓介 | 2022年9月28日 | |
| 一般社団法人 NationalClinicalDatabase(NCD)における手術・治療情報データベース事業 | 浜川博司 | 2022年1月17日 |
研究期間が終了した臨床研究
| 病理病期IA2-IIA期EGFR遺伝子変異陽性非小細胞肺癌における術後補助療法の実態を調査する多施設共同前向き観察研究 | 山田 徹 |
2024年9月17日 |
|
|---|---|---|---|
| EGFR遺伝子変異陽性非小細胞肺癌完全切除例の前向き観察研究 | 山田 徹 | 2025年2月4日 | |
| 重症COVID-19に対する人工呼吸管理中に発生した気圧障害の特徴と予後不良因子の検討 | 高橋 豊 | 2021年11月15日 | |
| 手術患者における入院前 COVID-19 スクリーニングの有効性についての研究 | 青山晃博 | 2020年5月20日 | |
| 高齢者肺癌に対する外科治療の安全性と有用性(多施設共同研究) | 高橋 豊 | 2015年7月3日 | |
| 高エネルギー胸部外傷患者における呼吸器系メカニクスに関する前向き研究 | 浜川博司 | ||
| 間質性肺炎合併肺がん切除患者における術後急性増悪予測スコアバリデーションスタディ REVEAL-IP(多施設共同非介入前向き研究) | 高橋 豊 | 2016年9月30日 | |
| 肺癌に対するサルベージ手術の有効性と安全性を検討する多施設共同後ろ向き臨床研究 | 高橋 豊 | 2017年8月15日 |
お知らせ
医師、医師を目指す方向け当科のご紹介
はじめに 〜「呼吸器外科」って何をしているの?〜
内科、外科、救急科…いろいろな科がある中で、「呼吸器外科」のページに入っていただき、ありがとうございます。
「呼吸器で手術…っていうと、肺癌と、気胸?教科書では…ページって、たったこれだけ?」くらいで、あまり馴染みのない診療科かもしれませんが、実は知れば知るほど奥が深く、重要な科です。
では、呼吸器外科の守備範囲は、どこでしょう? …答えは、心臓・大血管、食道、乳腺、脊椎・鎖骨を除いた胸部のすべてです。
つまり、肺、気管をはじめ、胸骨・肋骨、縦隔、胸膜・胸腔、胸郭の皮膚軟部組織などです。対象疾患は細かく挙げるとキリがありませんが、なぜこれだけ範囲が多岐に渡るのに、あまり知られることがないのか。 それは、「専門性が高すぎる」から。
私たちはこの領域のプロフェッショナルとして一人でも多くの患者さんのお役に立てるよう日夜診療にあたっています。もし興味を持たれたら、一度その現場を覗いてみるのはいかがでしょうか。今まで見えてこなかったものが見えてくるかもしれません。
当院の特徴
①日本有数の症例数
代表的な手術症例は、原発性肺癌、転移性肺腫瘍、縦隔腫瘍(胸腺腫など)、気胸、膿胸、胸部外傷(肋骨骨折など)、手掌多汗症などです。全身麻酔症例は年間400例前後で、全国有数の症例数を誇ります。他院で手術困難とされた症例も当院に数多く紹介いただいています。また総合病院の強みを生かし、心・呼吸器疾患、糖尿病などの手術リスクを抱えた患者さんの手術も適応を考慮しながら積極的に施行しています。
②低侵襲手術
国内外で、昨今の外科手術のテーマは「低侵襲手術」です。当科は手術の低侵襲化に特に力を入れ、これまでも積極的に胸腔鏡下手術(Video Assisted Thoracoscopic Surgery; VATS)を取り入れてきましたが、ここ数年はReduced Port Surgeryとして1つの創部で手術を完遂するUni-Port Surgery(または2 Port)を施行しています。低侵襲手術は患者さんの術後の負担を軽減しており、予定入院の患者さんは術後経過良好で、3〜4日で退院しています。

また、最近はロボット支援下手術(Robot Assisted Thoracoscopic Surgery; RATS)も取り入れるべく注力してます。
③外傷・緊急手術
当院で最も有名な診療科は何と言っても救急科です。厚生労働省から発表される「全国救命救急センター評価」において、2022年も1位に選ばれ、9年連続の栄誉です。このような背景があり、当科では外傷を中心とした救急疾患を数多く受け入れています。適応ありと判断された場合は、速やかに手術を行っています。
専攻医の研修先を考えている方へ
これから専攻医に上がる先生たちの最も気になることは、「どれだけの経験が積めるのだろう?」ということでしょう。
当院は数ある市中病院の中でも特色のある施設です。そんなところだとなかなか自分には執刀など回らないのでは?と思うかもしれませんが、専攻医の初めからしっかり回ってきます。もちろん不慣れな間はスタッフが力になります。スタッフは皆経験豊富で、科内は相談しやすい雰囲気が醸し出されています。
救急疾患は専攻医が中心に担当しており、主治医としての実力が養成されます。
病棟管理で最も大切なのは他科との連携ですが、呼吸器内科をはじめとしてどの科との連携も風通しがよく、コンサルトしやすいです。病棟をはじめ、コメディカルも熱心なスタッフばかりで、とても働きやすい環境であると言えます。
病院全体としてAcademicな活動が盛んであり、論文・学会発表や臨床研究も行いやすい環境です。
このように、市中病院としては間違いなくトップレベルの環境であり、満足のいく研修を積むことができるでしょう。
呼吸器外科専門研修カリキュラムローテートのススメ(初期研修医向け)
外科研修というと、病棟では上級医や専攻医の後ろをついて回るだけ、手術では清潔にはなったものの手袋はまっさらで、立ったまま画面を眺めるだけ…そんな研修では何も身につきませんよね?
高度すぎる手技や管理はできませんが、基本手技である胸腔ドレーン挿入、ドレーン抜去、胸腔穿刺は希望があれば積極的に担当できます(もちろんスタッフが指導、バックアップします)。手術では機会があればカメラ持ちや閉創もできます。百聞は一見に如かず、と言いますが、「一トライ」は「百見」に勝るので、このチャンスを生かしてください。
胸部レントゲンの読影はどの診療科にも必要な技術ですが、呼吸器外科医は立位のみならず、座位・臥位の写真も読影するので、呼内・放科にも劣らぬ技量を持っています。胸腔ドレーンの管理は難しそうですが、手術で胸腔を観察していると、「胸腔内がこう、だからこうなる」と本質的な理解に近づきます。また、胸腔内の観察は胸部レントゲン・CTの読影にも役立ちます。
このような実りある外科研修を希望される方は呼吸器外科をローテートしてみましょう。
外科系志望ではなくとも呼吸器内科や救急科など胸腔ドレーン挿入をする可能性のある科を志望の先生は、胸腔内の解剖を直接見て勉強できるよい機会なので、ぜひローテートしてください。今後への糧になることを約束します。当然、呼吸器外科医志望者は大歓迎です!
呼吸器外科の魅力
原発性肺癌や転移性肺癌を根治できたり、内科的な管理では限界のある気胸・膿胸を手術で治したり、肺生検で診断がつくことで適切な治療方針がついたりと、私たちの手で患者さんの治療を大きく前進させることが最大の魅力です。
最近は特に肺癌領域では新規薬剤もたくさん登場し、今まで手術対象ではなかった患者さんを手術させていただくことも多くなりました。日々治療は進歩しており、勉強すべきことは尽きません。
確かに、うまくいくことばかりではありません。しかし、担当患者さんが元気になって退院したり、次の治療に進めたりするのをみると、「ああ、呼吸器外科医になってよかった」とやりがいを感じ、次の診療へのエネルギーをもらうことができます。
皆さんも、呼吸器診療の「切り札」となって、私たちと一緒に働いてみませんか?
※本コンテンツは、医師の方を対象とし、当医療機関についての理解を深めていただけるよう作成しているものであり、一般の方を対象とする宣伝・広告等を目的としたものではありません。
はじめまして、神戸市立医療センター中央市民病院呼吸器外科の高橋 豊(たかはし ゆたか)と申します。
当科では術後の患者負担を最小限にするため、手術の約95%を胸腔鏡下に行っております。昨年の肺がん手術は133例とコロナのために減りましたが、全例が胸腔鏡下手術でした。今回はその中でも、更に低侵襲性を追求した単孔式で行う胸腔鏡下の肺がん手術についてご紹介いたします。
また、総合病院の強みを活かし、他院では手術が困難とされた患者さんに対しても根治性・呼吸機能温存を考慮した治療を行っておりますので、今後の患者紹介のご参考にしていただければ幸いです。
高橋 豊
副院長
呼吸器外科 部長
肺がん手術について
ご存知のように、肺がんはがんの罹患数で3番目でも死亡数は最も多い予後不良ながんです。
治療としては手術の他、化学療法・放射線療法があり、特に後2者の進歩は著しいものがありますが、根治性に最も優れるのは、やはり手術です。そして、肺がんの基本手術は腫瘍部分のみを切除する部分切除ではなく、肺葉切除です。これは開胸、胸腔鏡でも、またロボット支援下手術でも同じです。進行肺がんでは今でも開胸することはありますが、胸腔鏡を併用するので創は5~10cmですみます。
なお、ロボット支援下手術も胸腔鏡下手術の一種です。
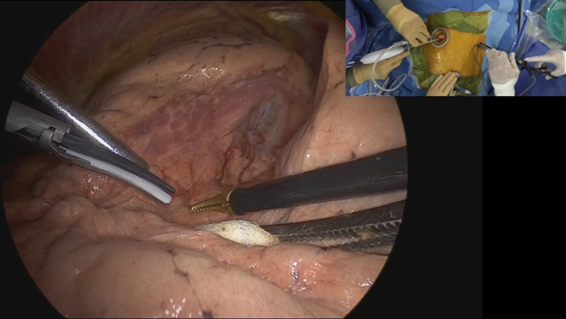
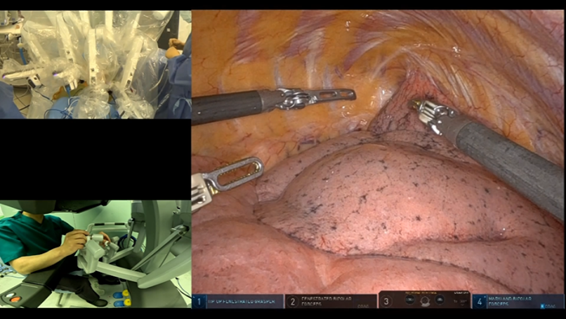
通常の胸腔鏡下手術は2~3cm大の創(ポート)3個で行うのが主流で、各ポートから胸腔鏡、自動縫合器をはじめとする器具を挿入して手術を行います。ロボット支援下手術は、拡大した立体視で、人では不可能な可動域を有し、手振れ補正も施した機器を使って手術するなど、数々のメリットがあります。しかし、今の機器では、最低でも5個の術創(ポート)が必要で、通常の胸腔鏡手術より創は多くなってしまうのが最大の欠点です。
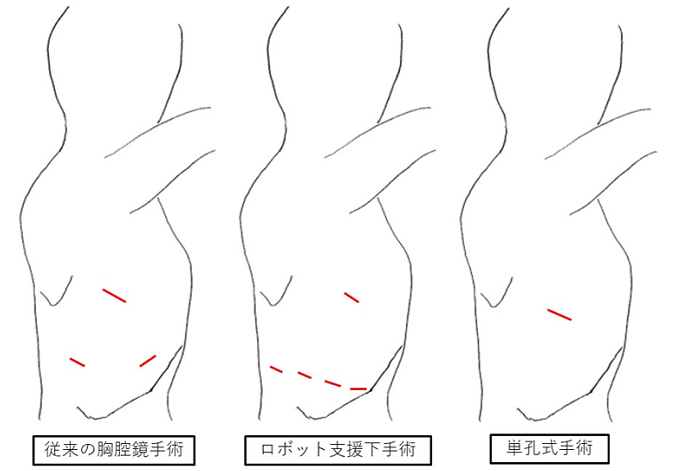
今回ご紹介する単孔式は、創を1個または2個で手術を行う方法で、一つまたは二つのポートから胸腔鏡や器具を挿入して行います。そのため、術創は3cm大が1個のみまたは、1cm大を追加する程度でより低侵襲で患者負担を軽減できる術式です。一方で、少ないポートでの行う手術となるため、通常より径の細い胸腔鏡や器具を操作する高い技術力を要し、術者と助手の息の合った連携が要求されます。当院では2個の術創で行う肺がん手術を2年前から始め、症例を選んで1個のみの術創で施行しています。
単孔式手術は一つのキズから胸腔鏡、手術器具を挿入して手術を行う
より低侵襲な手術です
呼吸器外科手術における術後疼痛は術中に生じた肋間神経の障害に起因するもので、いくら創が小さくても複数の肋間にポート孔を設ければ痛みは強くなります。当科では創が2個の場合でも同じ肋間に設けますので、痛みが軽減されます。このため、術翌日から食事や歩行が可能で、また、術創は吸収糸による埋没縫合を行いますから抜糸も不要です。早い方では術後2、3日で退院しており、昨年の平均術後在院日数は4.0日でした。
通常胸腔鏡下手術、ロボット支援下手術、単孔式手術の術創模式図
単孔式は脇の下に3cm大のキズで手術を行います。
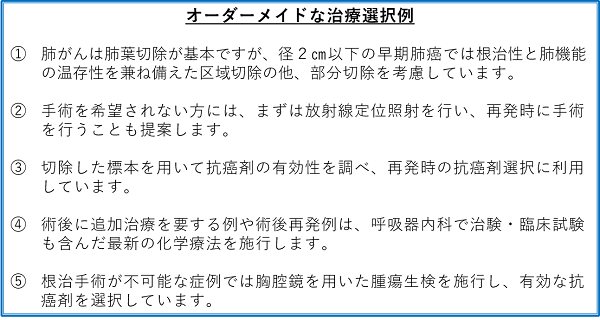
当院における肺がん診療 ~オーダーメイドな治療選択~
当院では、肺がんの治療方針は呼吸器内科・外科、放射線治療科による合同カンファレンスで検討し、3診療科が連携して診療にあたります。進行肺がんでは手術単独で治療が完結することは少なく、術前後に抗癌剤投与や放射線療法を行うなど、オーダーメイド的な治療に取り組み、治療成績の向上に努めています。以下にその例を示します。
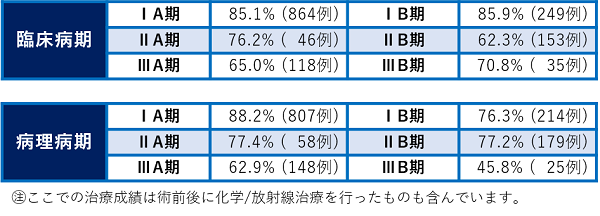
2011~2020年の肺がん治療成績(5年生存率)
当科の診療実績 ~他科と連携し、合併症にも対応~
重症な呼吸器・循環器疾患を合併、心臓の手術後などの理由から、他院では手術が困難とされた患者さんに対しても、総合病院である強みを生かして呼吸器内科・循環器内科など他科の協力のもと、根治性・呼吸機能温存を考慮した術式で、肺がんをはじめとする呼吸器疾患の治療にあたっています。
2020年の総手術数319例のうち、300例を胸腔鏡下手術で実施
2011年以降、手術件数は増加傾向でしたが、昨年は新型コロナウイルス感染拡大の影響を受け、手術総数は減少しました。前述の通り、当科では術後の患者負担を最小限にするため、全手術の約95%にあたる300例で胸腔鏡下手術を実施しており、あらゆる疾患に対応しております。
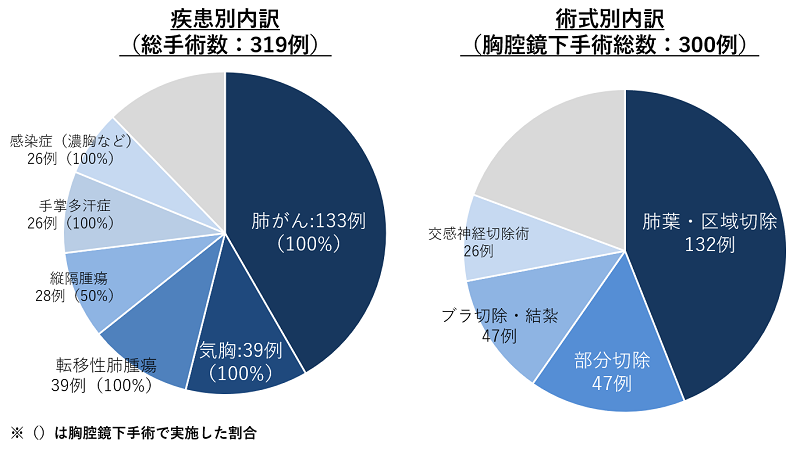
転移性肺腫瘍や良性腫瘍は部分切除が第一選択ですが、大きさや位置により部分切除が困難な場合は、肺葉・区域切除を施行します。
胸腔鏡下の肺葉・区域切除は難易度の高い術式ですが、当院では積極的に実施しており、胸腔鏡下手術の約半数を占めています。
あらゆる呼吸器疾患に対して低侵襲な手術を
肺がんを中心にご紹介してきましたが、以下の疾患に対しても低侵襲手術を迅速に提供しています。
・気胸
若年者に多いイメージがありますが、若い人だからこそ、早期の社会復帰が望まれます。術後は1~2日で退院可能な疾患ですので、手術までの期間を短くすることが肝要です。麻酔科・手術室の協力もあって、気胸は準緊急的に手術を行い、早期の退院を図っています。この他、手術困難な難治性気胸のご紹介も数多く受けております。
・膿胸
抗生剤やドレナージなどの内科的治療では治癒に時間がかかるうえに、なかなか完全な治癒も見込めません。早期に胸腔鏡下手術で膿を掻爬して洗浄に有効な位置にドレーンを置いて術後に洗浄すれば、治療期間の大幅な短縮、そして肺の十分な再膨張も得ることが出来ます。特にこの手術ではタイミングが重要ですので、気胸以上に緊急的に手術を行っています。
・他臓器がんの肺転移
原発性肺癌と異なり、部分切除が第一選択となります。しかし、これが困難な時は肺葉切除を要しますが、このような症例でも出来るだけ肺機能を温存すべく、胸腔鏡下の区域切除に取り組んでいます。
・縦隔腫瘍・重症筋無力症
積極的に胸腔鏡下手術を行っており、これらの疾患ではロボット支援下手術のメリットが大きいので、同手術を導入しております。
・手掌多汗症
皮膚科の先生方から症例を多くご紹介を頂き、胸腔鏡下に交感神経切断術を行っています。全身麻酔を要するため、1泊2日の入院は必要ですが、手掌多汗で悩まれている若い患者さんに喜ばれています。
年間400件近い手術をスタッフ3名、後期研修医3名で行っています。

当院のコロナ対策と診療状況について
当院では重症コロナ患者の診療にあたっているためか、一般診療を控えているかのような誤解が一部にみられます。コロナ患者は新造の別館で診療しており、一般患者と導線の交わることはありません。また、緊急入院も含め、本館入院患者にはPCR検査を入院時に全例行い、予定手術やエアロゾルの生じる検査(肺機能・気管支鏡検査など)を受ける患者には2週間前から症状日誌も記載してもらっています。徹底した感染管理によりウィルスの持ち込みを防いでいますので、肺がんに限らず、全ての疾患を安心して当院で治療を受けてもらうことが出来ます。
先生方へのメッセージ
肺がんの確定診断は腫瘍組織を採取して病理的に検討して得られるので、ご紹介の段階では画像診断のみがほとんどです。また、遠隔転移のないことが手術適応の条件ですので、手術可能かどうか判断しがたい症例も多くみられます。そのような場合でもお気軽に当院へご紹介ください。呼吸器外科・内科は密な連携で診療にあたっておりますので、当科のみでは対応困難な時でも、当科から呼吸器内科にコンサルト致します。
肺癌術後でも、術後に追加治療不要な経過観察のみの患者さんは、地域の先生方と一緒に診させて頂いております。当科では半年から1年に1回CT・PETなどで再発チェックを行うのみですので、その間は地域の先生に引き続き、診療して頂ければ幸いです。地域連携パスにつきましては「兵庫県がん診療連携協議会」のホームページ内にある「兵庫県がん地域連携パス」(http://www.hyogo-ganshinryo.jp/critical_path/index.html)をご参照ください。呼吸器を専門とされない先生でも使用できるパスとなっております。
肺がんを主に述べて参りましたが、その他の疾患もご紹介頂ければと存じます。

