
当院は神戸市の基幹病院として市民の生命と健康を守るために、患者中心の質の高い医療を安全に提供することを基本理念としていますが、特に循環器疾患(心臓や血管の病気)は生命と直結し待ったなしの対応が必要となる領域です。当科では、成人の循環器領域のあらゆる疾患に対して、緊急手術を含めて迅速に対応ができる体制をとっております。また、循環器センターとして、循環器内科と心臓血管外科が緊密に連携をとり、手術が検討される患者さんに対しては、循環器内科と心臓血管外科の合同カンファレンスで治療法を検討し、それぞれの患者さんに対して最適な治療法を提供できるように努めております。
手術に関しては、身体への負担ができるだけ少ない治療法、合併症の危険性ができるだけ少ない治療法であるとともに、安全・確実で、長期にわたって安心してすごしていただける治療法を提供できるように心がけております。カテーテル治療や低侵襲手術が適する場合があるのと同時に、長期にわたって安心してすごしていただくために従来通りの開胸や開腹手術が適した場合もあります。80歳以上の高齢者に対しても、心臓や大動脈の手術を含め、様々な臓器の保護に細心の注意を払って手術を行うことで、手術の安全性を高めております。
手術直後は、集中治療専門医と共に、治療を行なっております。必要に応じ、総合病院の利点を生かして、脳神経内科医・脳神経外科医・糖尿病内科医などの各診療科の医師が治療に加わります。また、医師だけでなく、看護師、臨床工学技士、リハビリテーション科スタッフ、薬剤師、栄養士、放射線科技師などの多職種でチーム医療を行なっております。
心臓の手術というと、怖い手術、大変な手術というイメージがあるかもしれません。しかし、最近は、手術手技が向上し、低侵襲手術もできるようになり、また、手術後の管理も向上し、高齢者の方も含めて、安心して手術を受けていただけるようになりました。生命に直結する病気のことも多く、恐れすぎず、頑張って手術を受けていただき、病気を乗り越えていただければ幸いです。手術後は、多くの方は元通りの生活ができます。必要以上に生活を制限せず、食事や運動などの生活習慣に気をつけながら、充実した生活を送っていただければ幸いです。
できるだけわかりやすく説明し、納得した上で治療法を決められるように努めたいと存じます。治療法の相談を含めてお気軽に受診ください。
弁膜症手術
大動脈弁狭窄症に対しては、年齢や合併疾患などを総合的に判断し、経カテーテル的大動脈弁留置術(TAVI)または従来通りの開胸での大動脈弁置換術を選択しております。80歳以上の第一選択は、経カテーテル的大動脈弁留置術ですが、合併疾患に対して同時手術が必要な場合などは、開胸での手術を行なっております。
僧帽弁閉鎖不全症に対しては、僧帽弁そのものが原因でおきる僧帽弁閉鎖不全症では、99%以上の症例で弁形成術を行なっております。心臓の機能や呼吸の機能に問題がなく、血管の正常が良好であれば、胸骨を切開せずに、小さい右開胸での手術(MICS)を行なっております。退院後の運動制限はなく、早期の社会復帰が可能となります。
心機能の低下した二次性僧帽弁閉鎖不全症に対しては、年齢や合併疾患を総合的に判断し、経皮的僧帽弁接合不全修復術(マイトラクリップ)または開胸手術を選択しております。
大動脈基部拡張症に伴う大動脈弁閉鎖不全症に対しては、人工弁に関係よる塞栓症や感染症などの合併症が避けられ、抗凝固薬(ワーファリン)の内服が不要な、自己の大動脈弁を温存する自己弁温存基部置換術を積極的に行っております。
冠動脈バイパス手術
冠動脈バイパス術の単独手術は、当院では90%以上の症例で、オフポンプ(人工心肺装置非使用、心拍動下)で施行しています。人工心肺装置にかかわる悪影響を回避でき、特に脳血管病変や腎機能障害を合併するハイリスク症例でそのメリットは大きくなります。
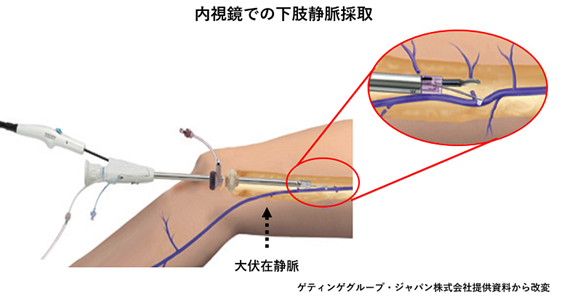
グラフト(バイパスに用いる血管)は、主に、内胸動脈と大伏在静脈を用いています。若年者には、長期開存性が良好な内胸動脈を積極的に2本使用しています。大伏在静脈は、動脈グラフトに匹敵する良好な長期開存性が報告されている、周囲の組織をつけたまま採取するno touch techniqueで採取しております。従来通りの大きさの創部になってしまうデメリットがありますが、動脈グラフトに匹敵する長期の良好な開存性が報告されており長持ちするため、デメリットを上回ると考えております。足の動脈硬化(閉塞性動脈硬化症)を合併している場合などは、創部合併症をきたす可能性が高くなるため、内視鏡を用いて小さな切開のみで採取しております。
大動脈手術
病変部位や合併疾患、年齢などを考慮して、開胸・開腹による人工血管置換術と、ステントグラフト内挿術を選択しております。80歳以上の高齢者に対しても、様々な臓器の保護に細心の注意を払って手術を行うことで、手術の安全性を高めております。救命救急センターをもつ神戸市の基幹病院として、大動脈瘤破裂や急性大動脈解離の緊急手術を数多く行なっております。
末梢血管手術
閉塞性動脈硬化症に対する下肢バイパス手術では、長期の開存性が良好な自家静脈をできるだけ使用するようにしています。重症な血流不足の原因となることが多い下腿病変に対しても、自家静脈を用いて下腿や足の血管へのバイパス術を積極的に行い、下肢の切断の防止に努めています。総大腿動脈病変などでは、内膜摘除術を行なっております。また、急性動脈閉塞に対する血栓除去術、維持透析のための内シャント造設術も施行しております。下肢静脈瘤に対しては、病変や患者さんの希望に応じて、血管内焼灼術、血管内接着剤治療(グルー治療)、非常に小さい皮膚切開での静脈瘤切除(スタブ・アバルジョン法)、高位結紮術、硬化療法を行っています。
診療実績
主な診療対象疾患
- 狭心症・心筋梗塞:冠動脈バイパス術、心室瘤切除術、左室形成術、左室自由壁破裂修復術、心室中隔穿孔修復術
- 弁膜症:大動脈弁置換術(開胸)、TAVI(経カテーテル的大動脈弁留置術)、僧帽弁形成術、
僧帽弁置換術、三尖弁形成術、三尖弁置換術、MICS(右小開胸手術) - 不整脈:メイズ手術、肺静脈隔離術、左心耳切除術・左心耳閉鎖術
- 心臓腫瘍(粘液腫など):心臓腫瘍摘出術、MICS心臓腫瘍摘出術
- 先人先天性心疾患:心房中隔欠損閉鎖術、心室中隔欠損閉鎖術
- 収縮性心膜炎:心膜切除術
- 大動脈瘤・大動脈解離:人工血管置換術、ステントグラフト内挿術
- 閉塞性動脈硬化症:下肢バイパス術、内膜摘除術
- 急性動脈閉塞:血栓除去術
- 下肢静脈瘤:血管内焼灼術(高周波・レーザー)、血管内接着剤治療(グルー治療)、
静脈瘤切除(スタブ・アバルジョン法)、高位結紮術、硬化療法 - 内シャント造設術(透析用)
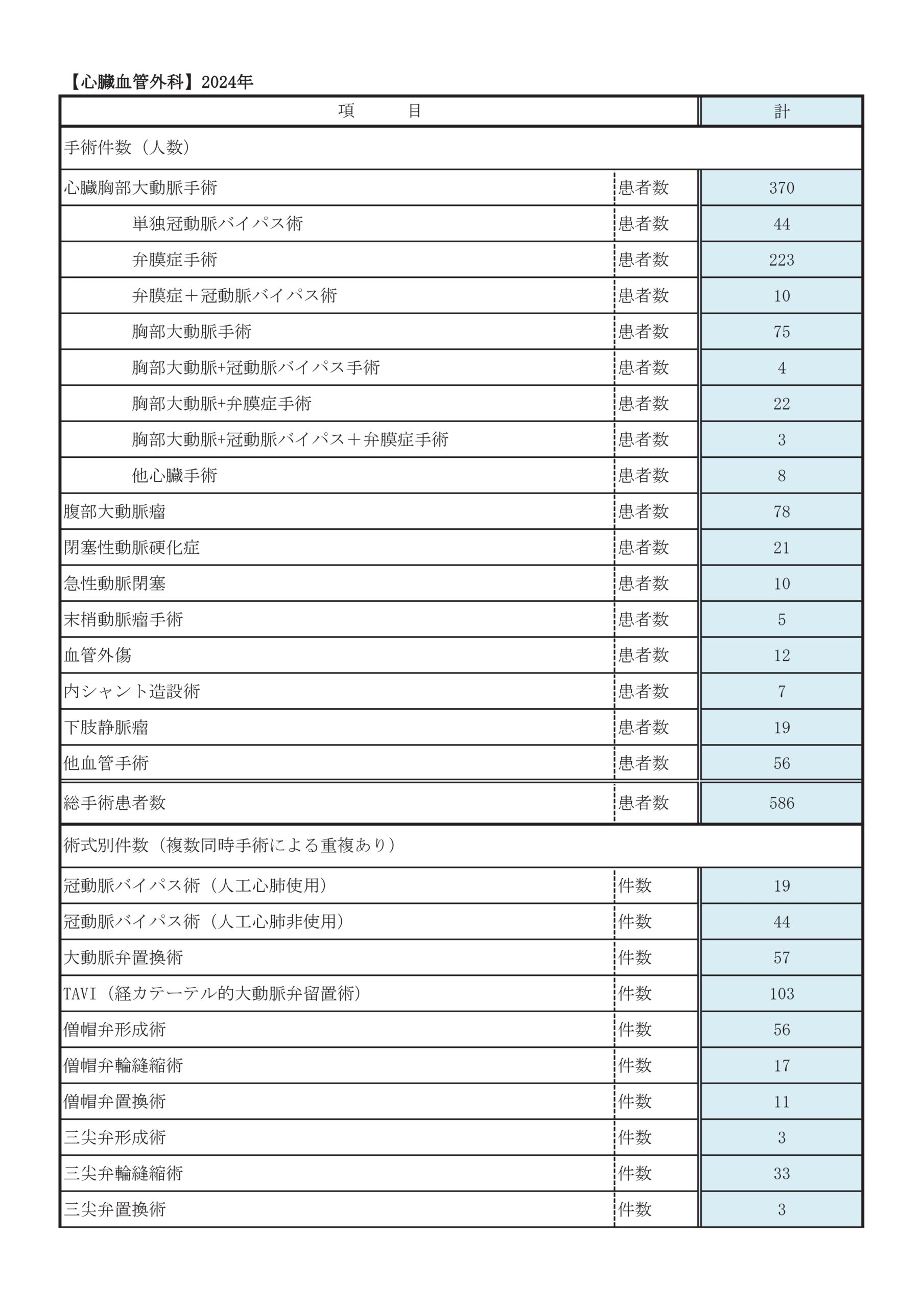
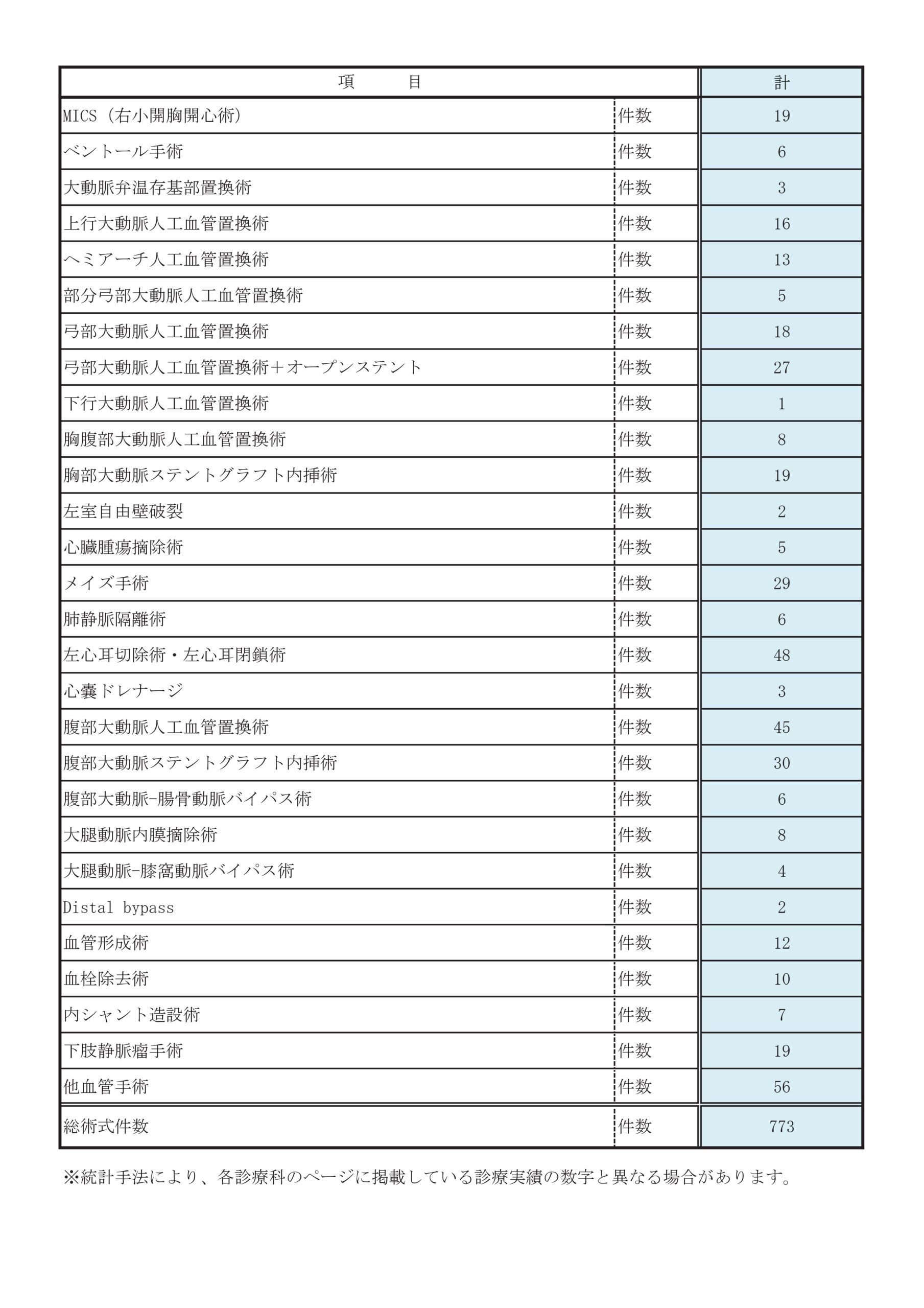
診療科別統計
主な疾患・治療法
冠動脈
①病気について
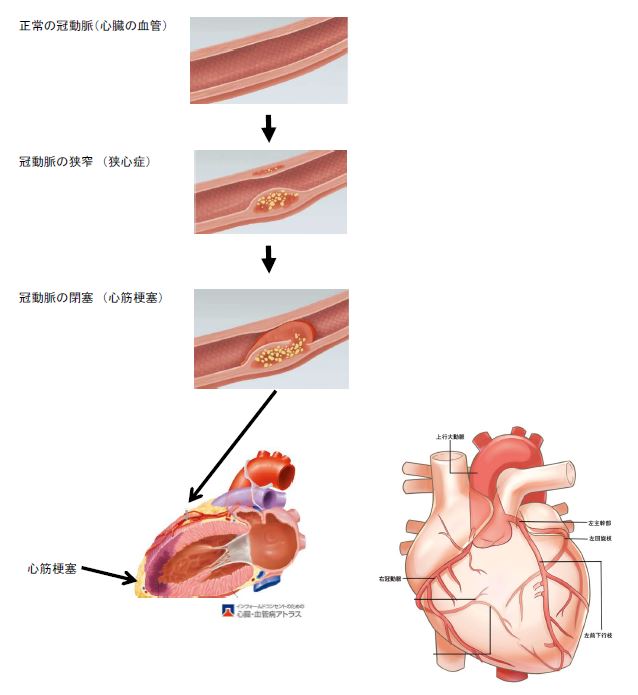
動脈硬化の塊が、 心臓の血管である「冠動脈」の壁に沈着し、冠動脈が細くなったり閉塞したりすることを総称して「虚血性心疾患」と呼びます。心臓の筋肉「心筋」への血流が低下した状態を「狭心症」、心筋への血流が完全に途絶え、心筋が壊死した状態を「心筋梗塞」と呼びます。糖尿病などの方は、症状がでないこともあり、「無症候性心筋虚血」と呼びます。動脈硬化とは、高血圧・高コレステロール血症・糖尿病・喫煙などの生活習慣病により、血管内にコレステロールやカルシウムなどが沈着した状態のことです。
急性心筋梗塞を発症すると、約10%の方は生命にかかわります。また、生命にかかわらずとも、障害を受けた心筋が機能しなくなるために心臓の機能が低下し、心不全の原因となったり、不整脈の原因となったりします。
②治療法
(1)薬物治療
病気が進行した場合、カテーテル治療(経皮的冠動脈形成術)や冠動脈バイパス術が必要になります。
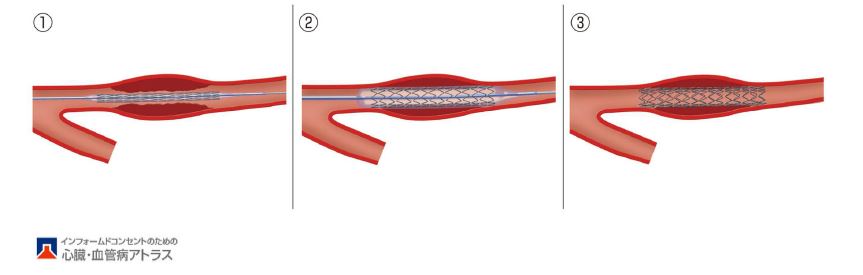
(2)カテーテル治療 (経皮的冠動脈形成術)
カテーテル(細い管)を用いて、風船やステント(金網)にて、細くなっている冠動脈や閉塞している冠動脈を拡張させ、血流を改善させる方法です。カテーテル治療は、冠動脈バイパス手術に比べて身体への負担が少ないです。循環器内科にて行っております。
(3)冠動脈バイパス術
身体の別の部位より血管を取り、細くなっている部位や閉塞している部位より先の冠動脈につなぎ、心臓への血流を改善させます。左冠動脈主幹部病変(左冠動脈の根元の病変)・左前下行枝近位部病変(左前下行枝の根元の病変)・3枝病変(3本の冠動脈全てに病変がある場合)・高度石灰化病変(冠動脈が非常に硬い場合)・びまん性病変(冠動脈の病変が長い場合)の方や、糖尿病の方、心臓の機能が低下した方の場合、カテーテル治療よりもバイパス手術のほうが、より長持ちし、長期的に心筋梗塞になる危険性がより下がり、寿命がより長くなります。
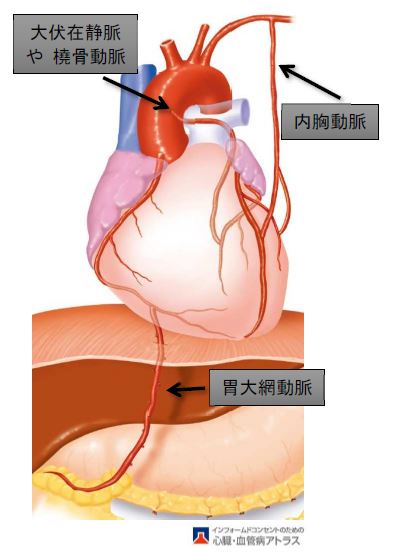
胸の動脈(内胸動脈)、足の静脈(大伏在静脈)、手の動脈(橈骨動脈)、胃の動脈(胃大網動脈)などを採取し、細くなっている部分や閉塞している部分より先の冠動脈につないで、心臓への血流を改善させます。
胸の動脈(内胸動脈)は、長期的に最も長持ちする血管で、当科では2本の内胸動脈を積極的に使用しています。足の静脈(大伏在静脈)は、当科では、良好な長期開存性が報告されている、周囲の組織をつけたまま採取するno touch techniqueで採取しております。
当科では、約90%の症例で、人工心肺装置を使用せずに(オフポンプ)冠動脈バイパス術を行っています。弁膜症の手術や胸部大動脈の手術が同時に必要な場合では、人工心肺装置を使用して手術を行います。
*人工心肺装置
人工心肺装置とは、心臓と肺の機能を持つ機械で、酸素を血液に取り込み、その血液を全身に送る機械です。弁膜症や胸部大動脈の開胸手術などで、必要になります。
弁膜症
①弁膜症とは
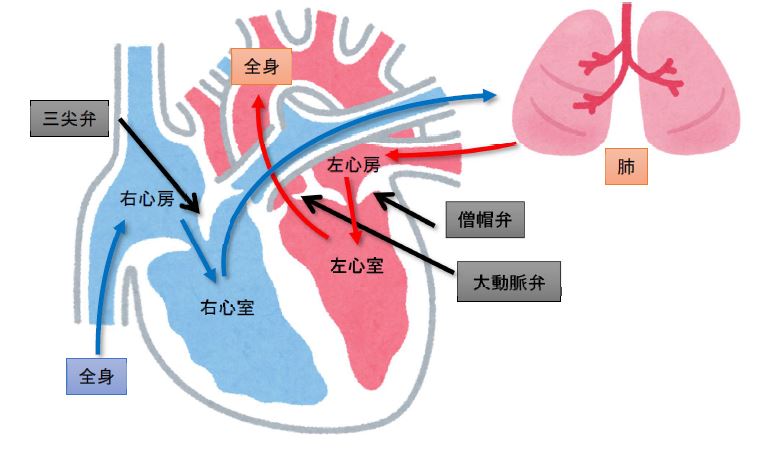
心臓には4つの部屋があります。
全身からかえってきた血液は、「右心房」→「右心室」→「肺」→「左心房」→「左心室」 の順に流れます。肺では、二酸化炭素を放出し、酸素を取り込みます。左心室より全身に血液が送り出されます。
それぞれの部屋には「弁」というドアがついており、血液が逆流しないように働いています。右心房の出口には「三尖弁」、右心室の出口には「肺動脈弁」、左心房の出口には「僧帽弁」、左心室の出口には「大動脈弁」がついています。
様々な原因で弁が機能しなくなった状態を「弁膜症」と呼びます。弁が十分開かなくなり血液が流れにくくなった状態を「狭窄症」と言い、また、弁がしっかり閉じないために血液が逆流する状態を「閉鎖不全症」と言い、心臓に負担がかかるようになります。弁膜症が悪化すると、心不全になり、息が苦しくなったり、顔や手足がむくんだりするようになります。
②治療法
(1)薬物治療
弁膜症が軽度や中等度の場合は薬物治療を行います。弁膜症が高度となった場合、弁形成術や弁置換術、TAVI(経カテーテル的大動脈弁置換術)を行います。
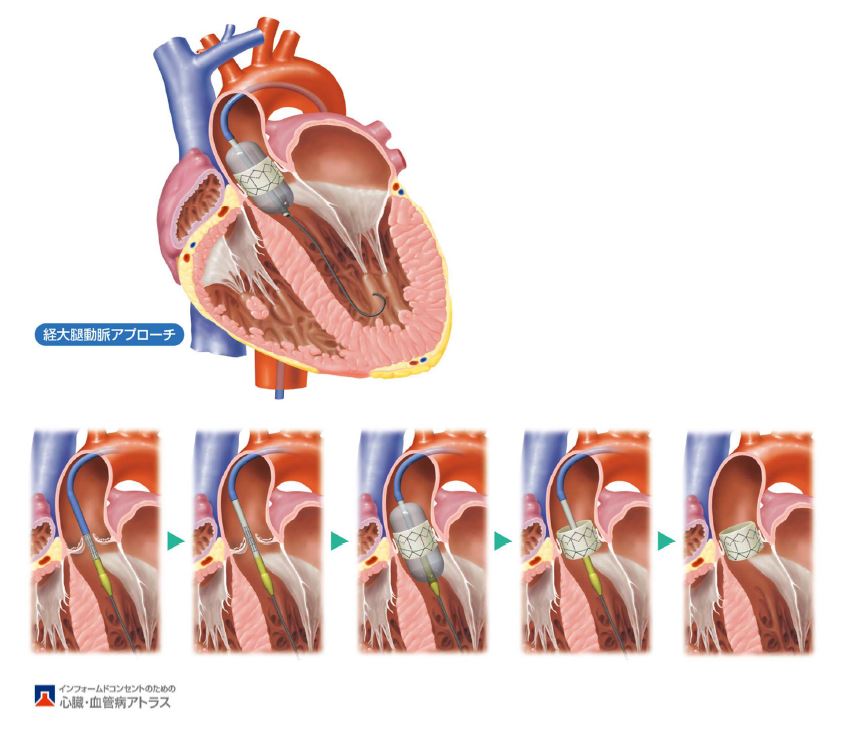
(2)TAVI(経カテーテル的大動脈弁置換術)
大動脈弁狭窄症に対して、胸を開かず、カテーテル(細い管)により人工弁を留置する手術です。胸を開かず、人工心肺装置も使用しないため、身体への負担が少ないです。人工弁の長期の耐久性がまだ不明です。
TAVIは、超高齢の方(80歳以上)、全身状態が不良の方、肺や肝臓の機能が高度に低下している方に適しています。
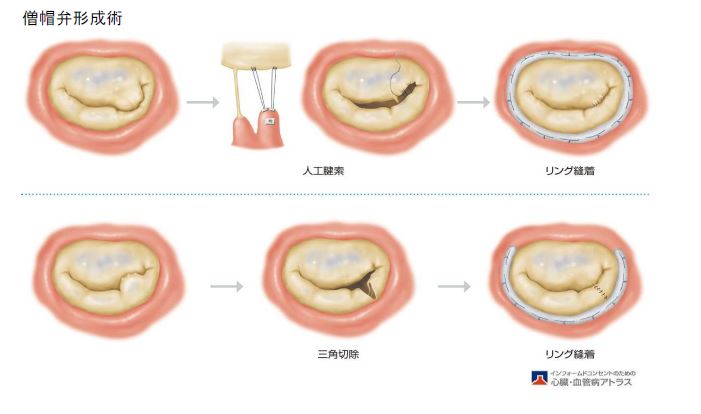
(3)弁形成術
開胸による手術には、人工弁に取り替える「弁置換術」と、ご自分の弁を修復する「弁形成術」があります。
「僧帽弁閉鎖不全症」に対しては、「弁形成術」の方が、心臓の機能が温存され、弁の感染が起きにくく、より長生きできると言われています。ただし、弁形成術を行った場合、逆流が残ったり、将来的に逆流が再発したりし、再手術が必要になる可能性があります。弁の破壊が強ければ、「弁置換術」が必要になります。
「三尖弁閉鎖不全症」の場合、ほとんどの場合「弁形成術」ができることが多いですが、弁の破壊が強い場合は「弁置換術」が必要になります。
(4)弁置換術
人工弁に取り替える手術です。特に、「大動脈弁狭窄症」、「大動脈弁閉鎖不全症」、「僧帽弁狭窄症」において、行われる手術です。
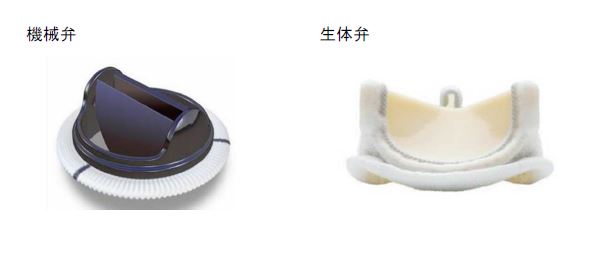
人工弁には、「機械弁」と「生体弁」の二種類があります。
「機械弁」は、カーボンでできており、耐久性が高く、より長持ちします。しかし、人工弁に血栓(血の塊)を作りやすく、血栓ができると脳梗塞が起きたり人工弁が働かなくなったりするため、血をさらさらにする薬(ワーファリン)を一生涯飲む必要があります。ワーファリンを飲むことにより、脳出血や、胃・腸からの出血などが問題になることがあります。
「生体弁」は、ウシの心臓の膜やブタの心臓の弁を用いて作られたものです。10~20年たつと、人工弁が劣化することがあり、再手術が必要になることがあります。心房細動など他の理由で必要がなければ、血をさらさらにする薬(ワーファリン)は手術後3ヶ月後に中止できます。
(5)右小開胸手術(MICS)
血管の状態が良好で、全身状態が良好であれば、右小開胸手術(MICS)により弁膜症手術を行なっています。
①心房細動とは
正常の心臓では、心房(右心房・左心房)→心室(右心室・左心室)の順番に、規則正しく心筋が収縮します。心房細動では、心房が非常に早く不規則に動く状態です。
心房細動となると、左心房の中で血液がよどみ、血の塊(血栓)ができやすくなり、脳梗塞などの原因となります。また、血液がよどむため、心不全になりやすくなります。
②治療法
(1)薬物治療
(2)電気的除細動
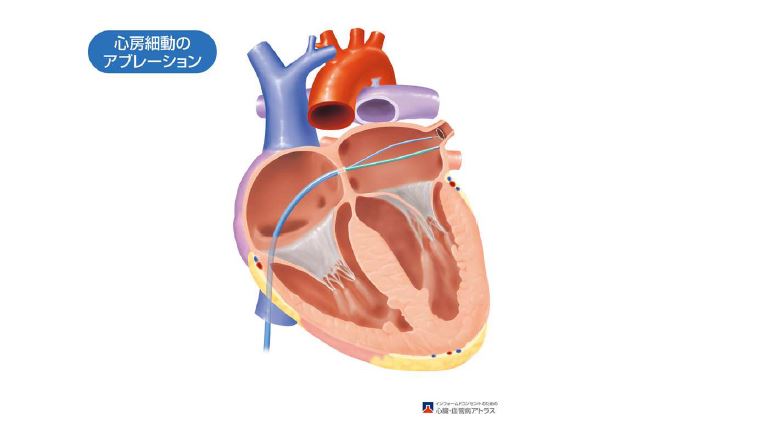
(3)カテーテルアブレーション
カテーテル(細い管)により、不整脈の原因となる心臓の電気回路を高周波や冷凍凝固で焼き切ります。循環器内科にて行っております。
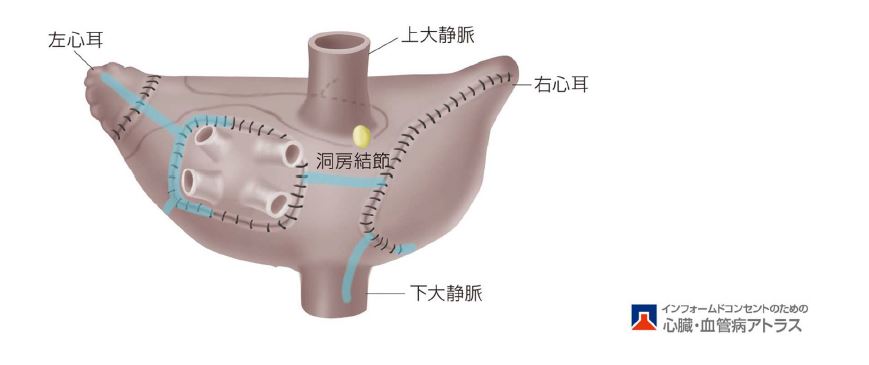
(4)メイズ手術、(開胸による)肺静脈隔離術
心臓手術を行う方で、心房細動を合併している場合、同時に不整脈手術を行うことがあります。不整脈の原因となる心臓の電気回路を高周波や冷凍凝固で焼き切ります。時々心房細動となる「発作性心房細動」では不整脈手術で治りやすく、長期間持続性に心房細動となっている「永続性心房細動」では治る確率がやや低くなります。
(5)左心耳切除術・左心耳閉鎖術
心房細動になると、左心房のうち耳のような形となった「左心耳」に、血の塊(血栓)ができやすくなります。血栓は脳梗塞の原因となるため、心房細動を合併された方の場合、左心耳を切除したり閉鎖したりして血栓ができにくいようにし、将来的な脳梗塞を予防する手術を行います。
大動脈疾患
①胸部大動脈瘤とは
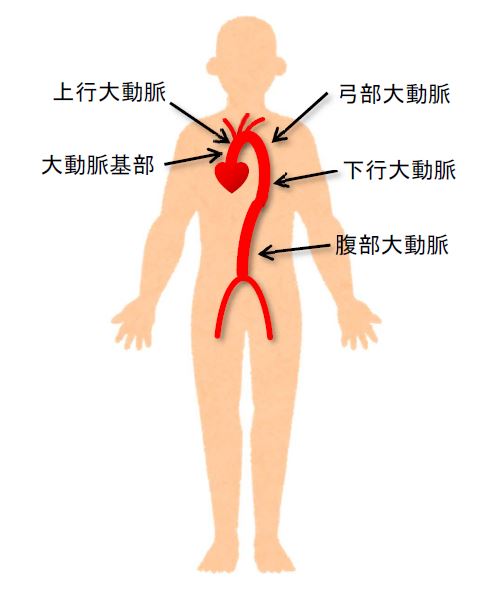
「大動脈」は、体の中で一番大きな血管で、心臓から送り出された血液の通り道です。
心臓から送り出された血液は、下記のように流れます。
↓
大動脈基部:心臓へ血管(冠動脈)を枝分かれします
↓
上行大動脈
↓
弓部大動脈:脳や腕に向かう血管を枝分かれします
↓
下行大動脈
↓
腹部大動脈:胃・腸・肝臓・腎臓に向かう血管を枝分かれします
↓
腸骨大動脈:足・腸・臀部に向かう血管を枝分かれします
胸の中の大動脈を総称して、「胸部大動脈」と言います。
大動脈が大きくなって「大動脈瘤」となると、破裂する危険性が高まります。大動脈瘤が破裂すると大量出血をきたし、多くの場合、病院にたどり着く前に生命にかかわります。また、破裂後に救急車で病院に運ばれても、状態が悪くなっていることが多く、緊急手術をしても救命率が低く、また、救命できても重篤な合併症が起きる可能性が高くなります。そのため、大動脈瘤がある程度大きくなった場合は、症状がなくても、破裂前に手術をする必要があります。
大動脈瘤の原因は、動脈硬化(糖尿病、高血圧、高脂血症、喫煙、加齢など)によることが多く、他の原因としては、解離、感染、炎症などです。
②治療法
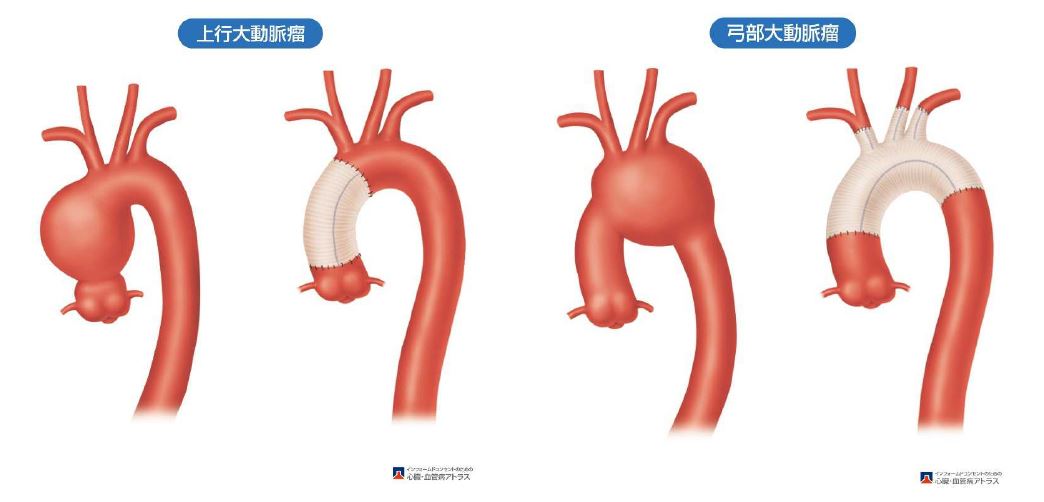
(1)(開胸による)胸部大動脈人工血管置換術
胸の中央又は左側を切開し、大動脈瘤を人工血管に取り替えます。
上行大動脈や弓部大動脈を人工血管に取り替える場合、心臓を停止させて手術を行う必要があり、代わりに「人工心肺装置」を用いて全身に血液を送り、心臓には心筋保護液という薬剤を注入して心臓を停止させます。また、各臓器(脳、心臓、腹部臓器や脊髄など)を保護するため体温を低下させて手術を行います。
*人工心肺装置
人工心肺装置とは、心臓と肺の機能を持つ機械で、酸素を血液に取り込み、その血液を全身に送る機械です。弁膜症や胸部大動脈の開胸手術などで、必要になります。
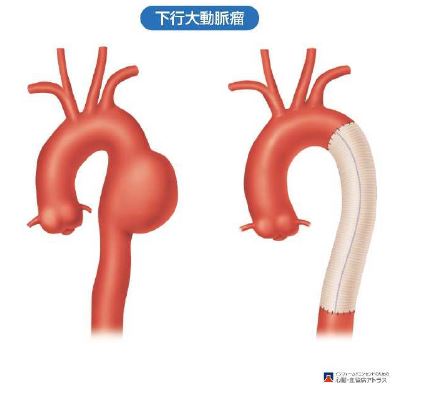
足の付け根を小さく切開し、カテーテル(細い管)を用いて、金網付き人工血管「ステントグラフト」を留置する方法です。開胸手術と比べ、身体への負担が少ないのがメリットです。下行大動脈瘤に適していることが多いです。上行大動脈瘤や弓部大動脈瘤には適していないことが多く、開胸手術が適していることが多いです

①大動脈解離とは
「大動脈」とは、体の中で一番大きな血管で、心臓から送り出された血液の通り道です。
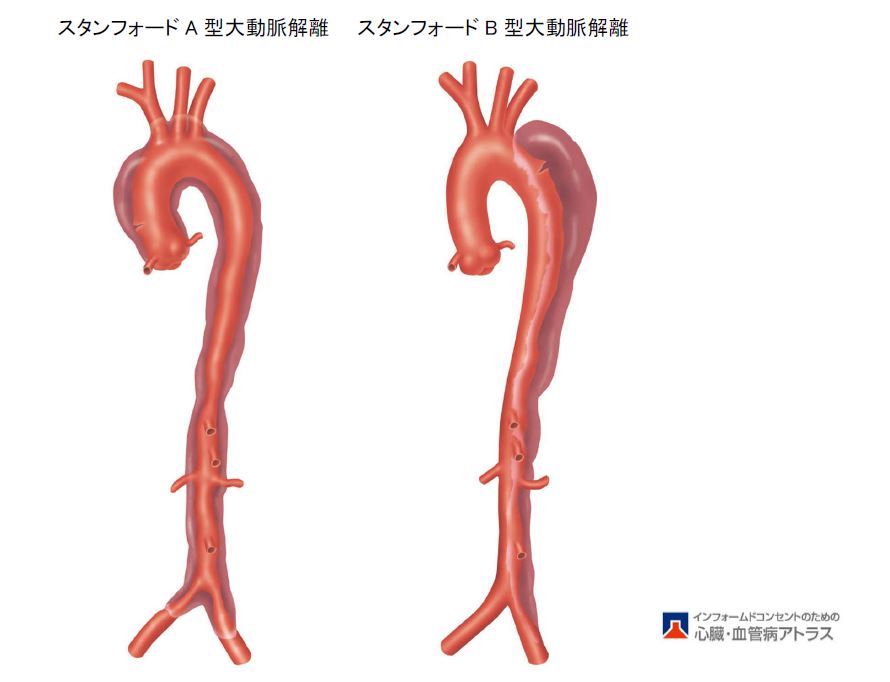
「大動脈解離」とは、大動脈の内側に亀裂が生じ、大動脈の壁が裂けて、壁の中に血液が流れ込んだ状態です。突然に発症することが多く(「急性大動脈解離」と呼びます)、大動脈の外側の壁が薄くなるために高い血圧に耐えられず大動脈が破裂する危険性があり、また、血管の壁が避けたために大動脈から枝分かれしている血管に血液が十分流れなくなって様々な臓器の障害(脳梗塞、心筋梗塞、手足の血流障害、腸の血流障害、腎不全など)が起こりうる病気で、生命にかかわる病気です。
上行大動脈に解離が存在する場合(スタンフォードA型大動脈解離)は、大動脈が破裂したり、心タンポナーデ(心臓の周りに血液がたまり心臓が圧迫されること)になったりしやすく、生命にかかわる可能性が高く、早期に手術が必要なことが多いです。心臓の出口についているドア「大動脈弁」に逆流をきたすことがあります。
上行大動脈に解離が存在しない場合(スタンフォードB型大動脈解離)は、急性期には血圧のコントロールと安静で経過を観察する場合が多いです。ただし、足や腸などへの血流が低下した場合や、大動脈が破裂した場合は、緊急の手術が必要になります。長期的には、解離した下行大動脈や腹部大動脈が拡大することがあり、ある程度大動脈が大きくなると破裂する危険性が生じ、手術が必要になります。大動脈の拡大を防ぐためには、血圧のコントロールが重要です。
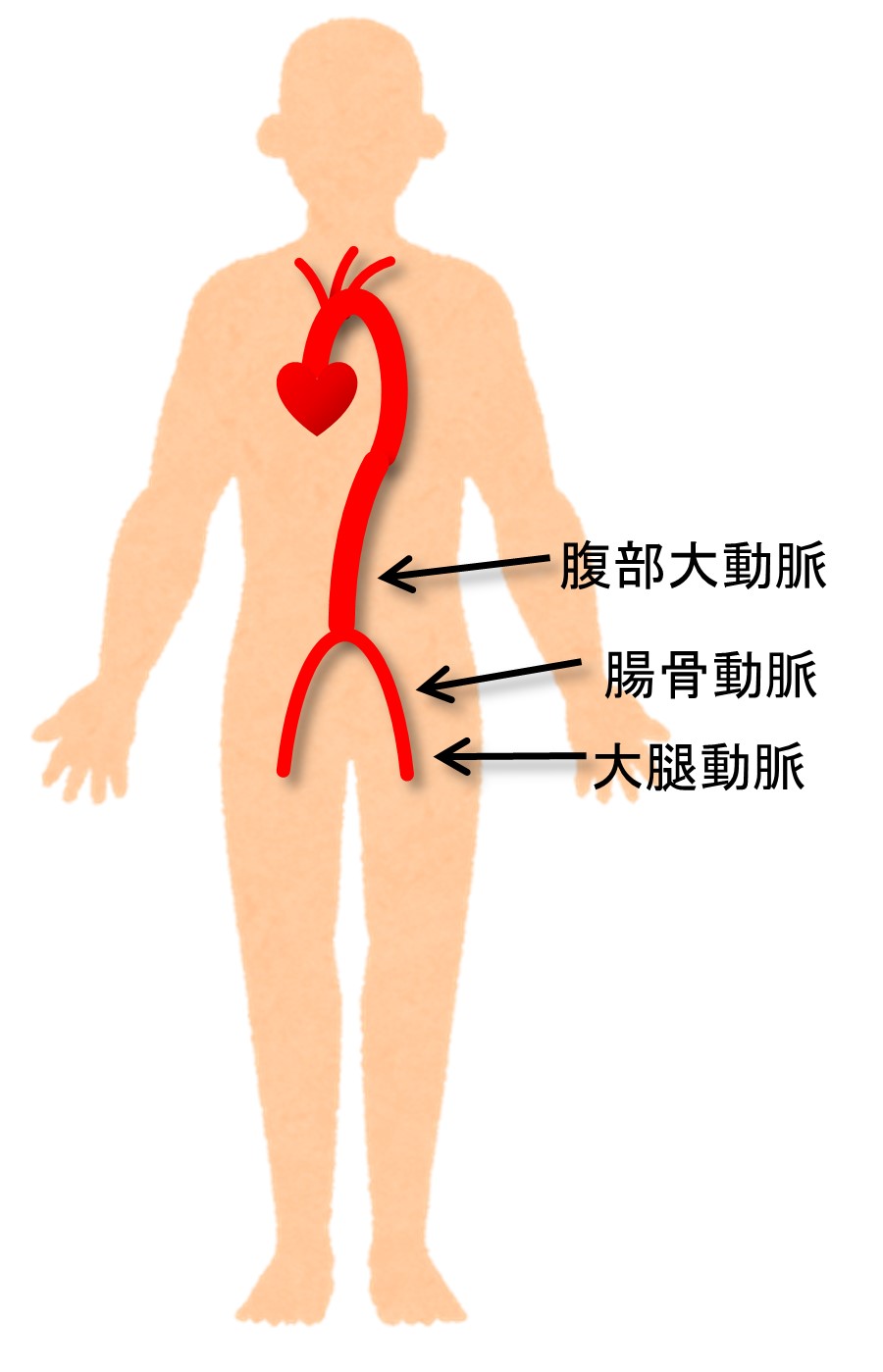
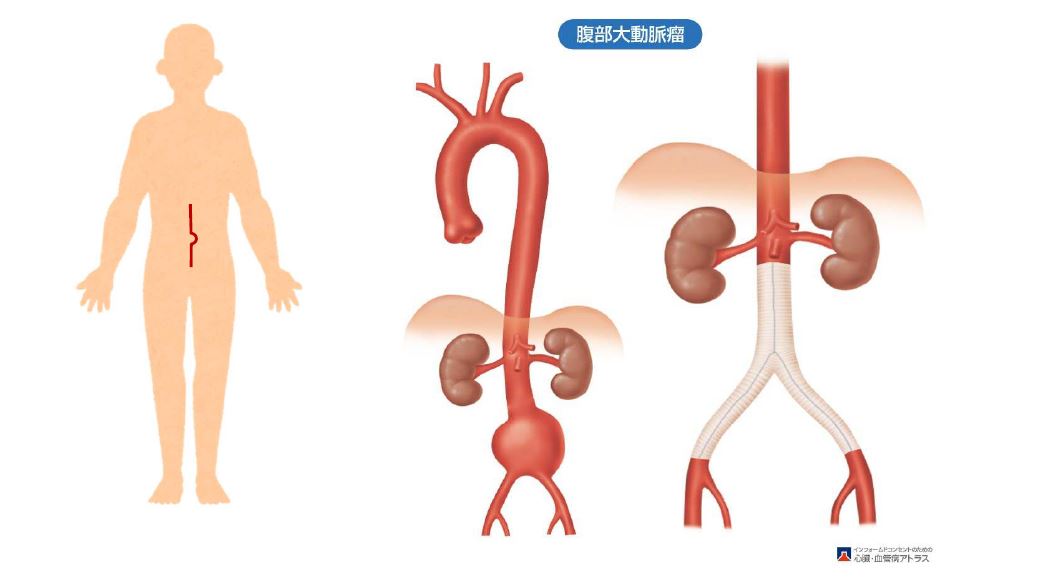
①腹部大動脈瘤とは
「大動脈」とは、体の中で一番大きな血管で、心臓から送り出された血液の通り道です。
血液は、腹部大動脈から足に向かって、下記のように流れます。
↓
腸骨動脈:腸・臀部に向かう血管を枝分れします
↓
大腿動脈:足に向かいます
大動脈が大きくなって「大動脈瘤」となると、破裂する危険性が高まります。大動脈瘤が破裂すると大量出血をきたし、多くの場合、病院にたどり着く前に生命にかかわります。また、破裂後に救急車で病院に運ばれても、状態が悪くなっていることが多く、緊急手術をしても救命率が低く、また、救命できても重篤な合併症が起きる可能性が高くなります。そのため、大動脈瘤がある程度大きくなった場合は、症状がなくても、破裂前に手術をする必要があります。
大動脈瘤の原因は、動脈硬化(糖尿病、高血圧、高脂血症、喫煙、加齢など)によることが多く、他の原因としては、解離、感染、炎症などです。
②治療法
(1)(開腹による)腹部大動脈人工血管置換術
腹部の中央を切開し、大動脈瘤を人工血管に取り替えます。
長期的に問題がおきることが少なく、治療が確実です。
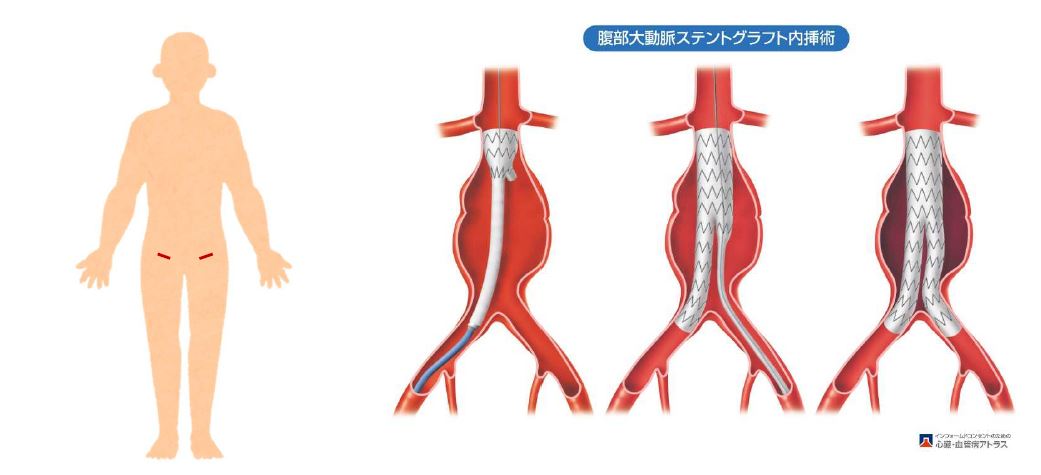
(2)腹部大動脈ステントグラフト内挿術
足の付け根を小さく切開し、カテーテル(細い管)を用いて金網付き人工血管「ステントグラフト」を留置する方法です。開腹手術と比べ、身体への負担が少ないです。
しかし、治療したにもかかわらず、将来的に腹部大動脈瘤が拡大することがあり、定期的な検査が必要です。大動脈瘤が拡大した場合、追加治療(カテーテル治療や開腹手術)が必要になります。
①閉塞性動脈硬化症とは
閉塞性動脈硬化症とは、動脈硬化により、足の血管が細くなったり、閉塞したりするために、足への血流が低下した状態です。動脈硬化とは、高血圧・高コレステロール血症・糖尿病・喫煙などの生活習慣病により、血管内にコレステロールやカルシウムなどが沈着した状態のことです。
休まずに長い距離が歩けなくなったり、進行すると安静にしていても足に痛みを認め、足の皮膚に潰瘍ができたり、さらに進行すると、足が壊死して足の切断が必要となる可能性があります。
②治療法
(1)運動療法
(2)薬物療法
(3)カテーテル治療
(4)バイパス手術
当科では、長期の開存性が良好な自家静脈をできるだけ使用するようにしています。重症な血流不足の原因となることが多い下腿病変に対しても、自家静脈を用いて下腿や足の血管へのバイパス術を積極的に行い、下肢の切断の防止に努めています。総大腿動脈病変などでは、内膜摘除術を行なっております。
①急性動脈閉塞とは
突然、手や足の動脈が閉塞し、痛み、蒼白、知覚鈍麻、運動麻痺などを認める病気です。手や足の切断が必要になる可能性が高く、早期の治療が必要です。
②治療法
(1) 血栓除去術
風船付きカテーテルで、血の塊(血栓)を除去する手術
(2) カテーテル治療
(経皮的血栓吸引療法、経皮的血管形成術、経カテーテル血栓溶解療法など)
静脈瘤
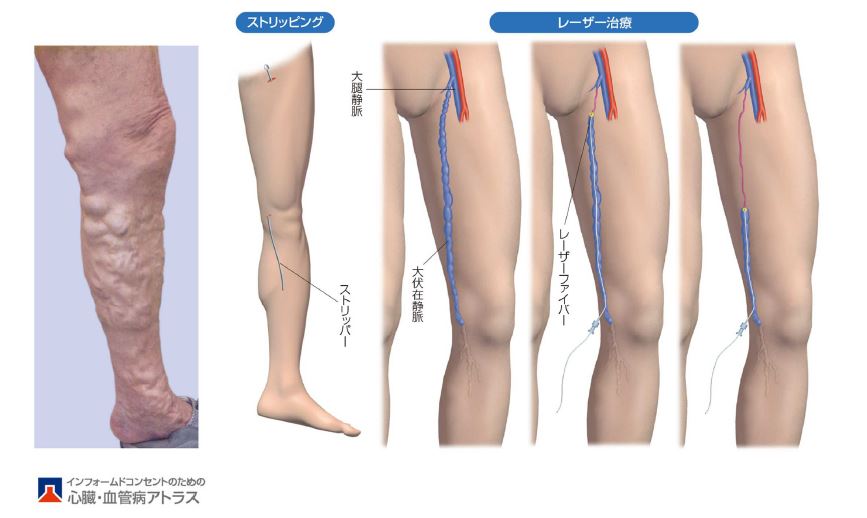
①下肢静脈瘤とは
全身から心臓へ戻る血液が通る道を「静脈」と言います。足の静脈には、足の奥深くを走行する「深部静脈」と足の表面を走行する「表在静脈」があります。通常、血液は、表在静脈から深部静脈に血液が流れ、その間には一方向弁がついていて、血液が逆流しないようになっています。一方向弁が壊れ、深部静脈より表在静脈に血液が逆流するようになると、表在静脈が拡張して「下肢静脈瘤」となります。足がだるくなったり、こむらがえりが起きたり、むくむようになったり、湿疹や色素沈着を認めたり、皮膚の硬化・皮膚の潰瘍を認めるようになります。
診断は超音波検査で下肢の静脈の状態を検査して行います。
治療は、軽症の場合は、生活習慣の改善や弾性ストッキングによる圧迫を行います。上記のような症状が出現した場合に手術を検討します。手術は日帰りもしくは1泊入院で行なっています。
診察日は毎週木曜日で当日予約も受け付けていますので、お気軽にご相談下さい。
②治療法
(1)血管内焼灼術
カテーテル(細い管)を逆流が起きている静脈に挿入し、静脈を高周波もしくはレーザーで焼いて、静脈を閉塞させ、血液が逆流しないようにする治療法です。
(2)血管内接着材治療(グルー治療)
カテーテル(細い管)を逆流が起きている静脈に挿入し、静脈内に接着材(グルー)を注入して、静脈を閉塞させ、血液が逆流しないようにする治療法です。
(3)静脈瘤切除術(スタブ・アバルジョン法)
皮膚を非常に小さく(1〜2mm)切開し、フックで静脈瘤を引っ張りだし、静脈瘤を切除します。
(4)静脈抜去術(ストリッピング手術)
血管内治療が適さない場合に、逆流している静脈を引き抜きます。
(5)高位結紮術
血管内治療や静脈抜去術が適さない場合に、静脈の根元をしばり、血液が逆流しないようにします。
(6)硬化療法
(7)弾性ストッキング
軽症の場合に用います
臨床研究
当科では臨床上の様々な疑問点を解決すべく臨床研究を行っています。観察研究とは直接の同意は頂かずこの掲示を持って同意して頂いたものとして実施されています。また院内の臨床研究倫理委員会にて審査・認可された介入研究や観察研究ではその対象となる患者さん個人に説明し同意を頂いた上で実施しています。
主な臨床研究(観察、介入研究を含む)
| 研究課題名 | 当院責任者 | 説明文 (PDF) |
| Stanford A型大動脈解離術後の中枢側仮性動脈瘤に対する手術の検討 | 江﨑二郎 | |
|---|---|---|
| 一般社団法人 National Clinical Database (NCD)における手術・治療情報データベース事業 | 江﨑二郎 | |
| 大動脈弁形成術に対する全国アンケート調査 | 江﨑二郎 | |
| 僧帽弁位人工弁周囲逆流に対する外科的修復術の遠隔成績 | 吉田一史 | |
| 僧帽弁閉鎖不全症に対する後尖patch augumentationの遠隔成績 | 吉田一史 | |
| 機能性重症三尖弁閉鎖不全症に対するFlexible bandによる弁輪縫縮の遠隔成績 | 吉田一史 | |
| 心臓原発肉腫に対する外科的切除後の局所再発の予防 | 吉田一史 | |
| 広範胸腹部大動脈瘤に対する胸部大動脈ステント内挿術と胸腹部大動脈人工血管置換術を組み合わせたハイブリット治療の有効性の検討 | 吉田一史 | |
| 重症虚血性僧帽弁閉鎖不全症に対する乳頭筋に介入した僧帽弁形成術の有用性に関する多施設共同研究 | 江﨑二郎 |
地域の先生方へ
当科では、成人の循環器領域のあらゆる疾患に対して、緊急手術を含めて迅速に対応ができる体制をとっております。また、循環器センターとして、循環器内科と緊密に連携をとっており、週2回循環器内科と合同カンファレンスを行い、個々の患者さんに最適な治療法の検討や、治療後の経過を共有し治療法の再検討をいたしております。あらゆる領域の専門医がいる当院の強みをいかし、さまざまな合併疾患を持った方に対して、各専門医と連携しながら治療を行っております。
80歳以上の高齢者に対しても、様々な臓器の保護に細心の注意を払って手術を行うことで、開心術を含めて手術の安全性を高めております。
手術適応に迷われる症例も含めて、お気軽にご相談いただければ幸いです。
江﨑 二郎
心臓血管外科 部長
当科へのご紹介方法と診療フロー
当科への紹介には当院ホームページに記載されているFAX予約もしくはWeb予約をご利用ください。Web予約ではこちらから専用のIDとパスワードを配布しますので、そこから専用のサイトにアクセスして、空いている枠へ直接予約が可能となっています。
また、急がれる症例や、直接相談を希望される場合は、24時間いつでも対応可能となっています。
当院受診後は治療方針が決まり次第ご連絡を差し上げます。通常手術日の1〜2日前に入院していただき、術後10日〜2週間で退院となります。退院後2〜3ヶ月当科外来で術後経過を診させていただき、安定後に、ご紹介いただいた先生へ逆紹介させていただいております。
初期研修医・学生のみなさんへ
当科では、年間250〜300例の開心術(人工心肺使用症例+OPCAB)、約50例のステントグラフト内挿術、約50例の腹部大動脈人工血管置換術、100〜150例の末梢血管手術を施行しています。神戸市の基幹病院で救命救急センターを備え、神戸市の最後の砦として数多くの救急搬送を受け入れており、大動脈解離や大動脈瘤破裂などの緊急手術も豊富に経験できます。小開胸開心術(MICS)、ステントグラフト内挿術、経カテーテル的大動脈弁留置術(TAVI)などの低侵襲手術も経験することができます。末梢血管手術が豊富で、専攻医も執刀経験をつむことができます。
専攻医の教育プログラムは3年間となっております。当院では成人の心臓血管外科手術を豊富に経験できますが、3年間のうち半年間は尼崎総合医療センター心臓血管外科をローテートし、小児の心臓血管外科手術も経験することができます。外科専門医取得のため、他領域の外科手術を経験する必要がありますが、当院は全ての科で手術症例数が多いため、短期間で必要な経験をすることができ、3年間のうち多くの期間を心臓血管外科で研修することが可能です。
ICUは集中治療医がメインに管理をしており、手術により集中しやすい環境です。
働き方改革の取り組みとして、オンオフのメリハリをしっかりつけています。夜間・土日・祝日は、当番制としており、当番以外は緊急手術があっても休みとなります。緊急手術が多いですが、オフをしっかり取れる体制にしております。
カンファレンスは、火曜日は、隔週で大動脈カンファレンスと弁膜症カンファレンスを循環器内科と合同で行い、大動脈手術や弁膜症手術後の症例の振り返りを行なっています。水曜日は、循環器内科と症例検討会を行い、ハートチームとして症例毎に最適な治療方針を決定しています。木曜日は集中治療医とM&M、学会発表の予行練習、抄読会を行い、金曜日は、麻酔科医師・臨床工学技士・看護師とともに翌週の手術症例の術前カンファレンスを行っています。専攻医は、カンファレンスでプレゼンテーションを行うことで、プレゼンテーションのしかた、ガイドラインも含めた一般的な検査・治療・術式・術後管理などにつき学ぶことができます。
学会への参加や演題発表にも積極的に行う方針としています。学会で、最新の知識が得られるとともに、発表の準備に際して関連した知識を学ぶことができ、発表にてプレゼンテーションの機会がえられます。臨床研究に対する院内のサポート体制も充実しています。
他院で初期研修をされている先生の当科の専攻医プログラムへの応募も大歓迎です。お気軽に見学やお問い合わせをして下さい。

